Geriatric considerations - Respiratory: Nursing
Geriatric considerations - Respiratory: Nursing
HIT II Exam 1
HIT II Exam 1
Notes
| GERIATRIC CONSIDERATIONS - RESPIRATORY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
| RISK FACTORS |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Geriatrics is the branch of medicine that deals with the physiology and psychology of aging, as well as the diagnosis and treatment of diseases affecting older clients. Now, aging affects various organ systems, one of which is the respiratory system. All right, now let's start by reviewing the physiology of the respiratory tract, which can be divided into the upper respiratory tract and lower respiratory tract. The upper respiratory tract includes the nose, nasal cavity, the oral cavity, pharynx, epiglottis, larynx, and the upper part of the trachea; while the lower respiratory tract includes the lower part of the trachea, and the lungs, which contain the bronchi, bronchioles, alveolar ducts, and finally the alveoli.
Most of the respiratory tract is lined with a pseudostratified ciliated columnar epithelium, which contains goblet cells that produce mucus to trap small foreign particles; as well as columnar cells, which have cilia, or tiny little hair-like projections, that move mucus up the respiratory tract so it can trigger the cough reflex, and get coughed out. The cough reflex is also controlled by the central and peripheral nervous systems. Now, let’s follow air as it passes through the respiratory tract. First, it enters the nose, which humidifies and warms that air, before sending it to the pharynx. From the pharynx, air passes through the epiglottis, and enters the larynx. Next is the trachea, which ends at the carina by bifurcating into the right and left main bronchi, which get inside the lungs, where they gradually branch into smaller bronchi, and bronchioles. These bronchioles have smooth muscles in their walls that allow them to constrict or dilate in response to certain stimuli.
Bronchioles carry the air into alveolar ducts, and finally the alveoli, which are tiny sacs responsible for gas exchange between the air and the blood. Alveoli also have elastic recoil, which gives them the ability to stretch and rebound with each breath. Within the alveoli, there are alveolar macrophages, which swallow pathogens and foreign particles before they enter the bloodstream. Now, lungs are surrounded by the chest wall that consists of the sternum, ribs and their costal cartilages, in addition to thoracic vertebrae. Respiratory muscles are divided into primary and secondary respiratory muscles. Primary respiratory muscles are the diaphragm and external intercostal muscles, whereas secondary respiratory muscles include the sternocleidomastoid and abdominal muscles.
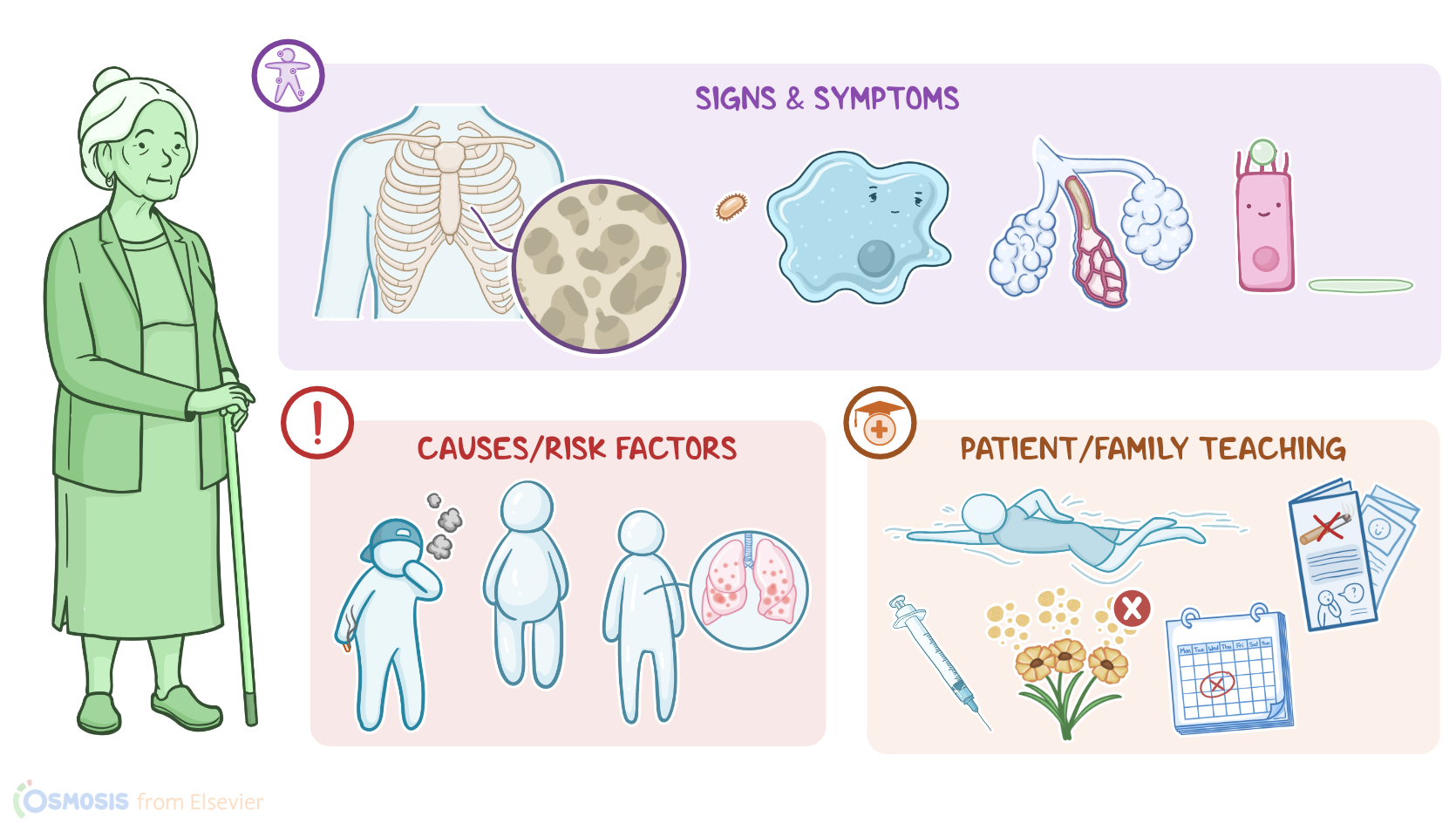
Effects of aging on the respiratory system include changes in structure and function. These changes include stiffness of the chest wall and decreased mobility of the ribs. Osteoporosis and calcification of costal cartilages also contribute to the rigidity of the chest wall. Effects of these changes include decreased chest expansion, inefficient deep breathing, and a less effective cough reflex. Additionally, the strength and mass of the respiratory muscles decline, and the elastic recoil of the lungs, as well as the conducting airways is reduced. These changes make it harder to inflate the lungs, which increases the work of breathing, and decreases exercise tolerance. Other changes include a decreased number of functional alveoli, which decreases the surface area available for gas exchange.