Guillain-Barré syndrome: Nursing
1,169views
Guillain-Barré syndrome: Nursing
Exam 1 Fall 2024 Pathophysiology Pre Nursing
Exam 1 Fall 2024 Pathophysiology Pre Nursing
Notes
| GUILLAIN-BARRE SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
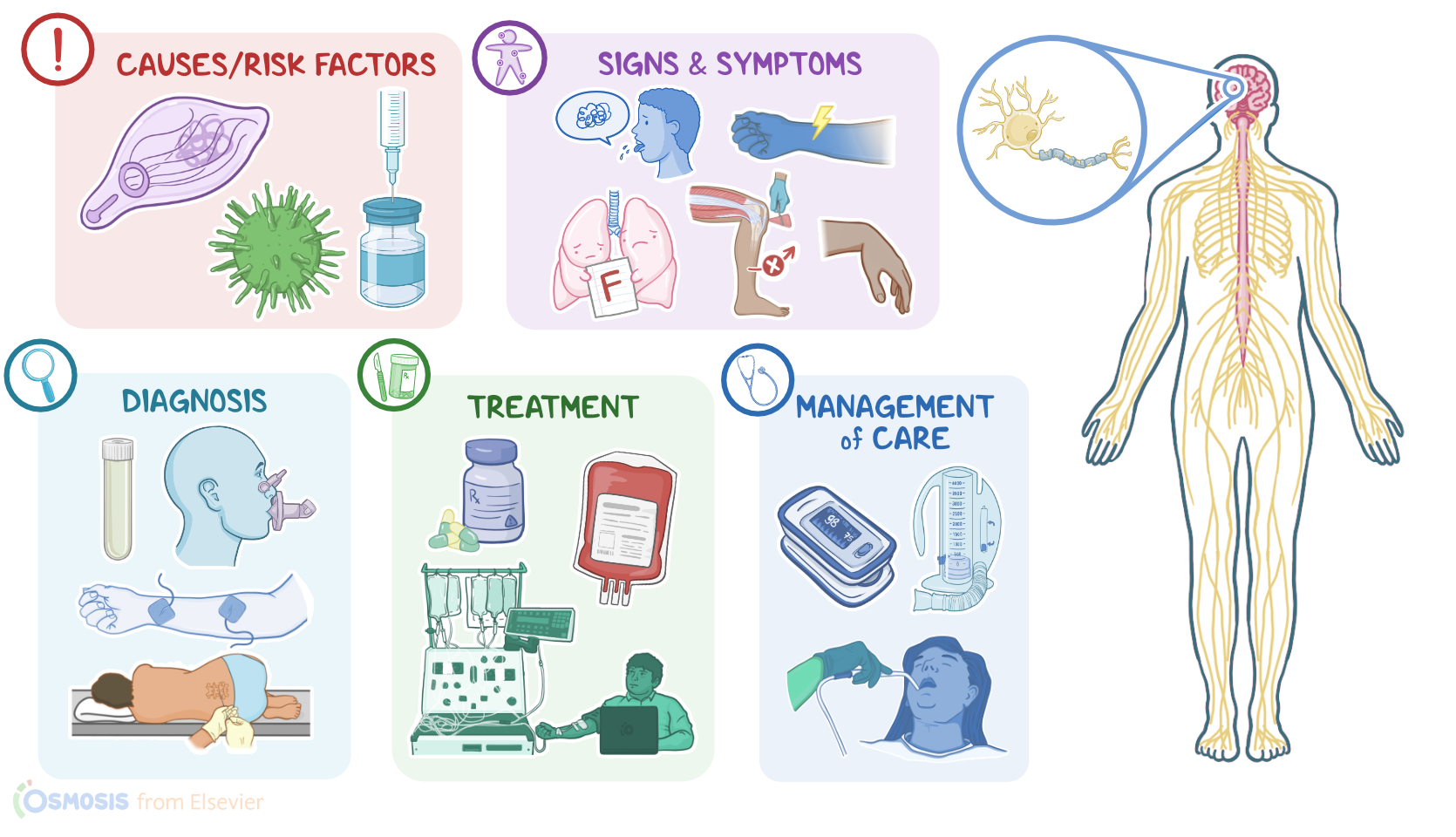
Guillain-Barré syndrome, or GBS for short, is a rare but potentially serious autoimmune disease characterized by acute demyelination and degeneration of the peripheral nerves, which ultimately leads to muscle weakness and even paralysis.
Now, let’s quickly review the anatomy and physiology of the peripheral nervous system, which includes all of the neurons that extend beyond the brain and the spinal cord. Neurons are made up of three main parts, the dendrites, cell body, and axon. The dendrites are little branches that receive nerve impulses, or signals from other neurons, and carry them to the cell body, which has all of the neuron’s main organelles.
The cell body then transmits the nerve impulse through the axon to the next neuron in the series.
The axons are surrounded by myelin, which is a fatty protective sheath that also helps speed up that impulse. This myelin is produced by Schwann cells, which are a group of cells that support neurons.
For peripheral nerves, the cell body can either be located in the spinal cord, and this is called a spinal nerve; or the brain, which is called a cranial nerve.
Alright, so Guillain-Barré syndrome is caused by demyelination of the peripheral nerves. The underlying cause of this demyelination isn’t clear, but there are some known risk factors and triggers, such as a recent bacterial infection, like Campylobacter jejuni and Mycoplasma pneumoniae, as well as a viral infection, like cytomegalovirus and Epstein-Barr virus, and in rare cases, clients may also develop Guillain-Barré syndrome soon after getting a vaccine, such as the flu vaccine.
Okay, now these bacteria and viruses don’t directly damage the myelin sheath. Instead, it’s thought that they have antigens on their surface that look similar to the lipids in the myelin sheath,
so immune cells and antibodies can mistakenly attack and destroy the myelin sheath surrounding peripheral nerves. As a result, nerve impulses become slow and sluggish, and ultimately, there’s degeneration of the peripheral nerves.
Signs and symptoms of Guillain-Barré syndrome typically occur days to weeks after the trigger, and they typically present with acute, ascending, bilateral weakness - that starts with the lower limbs, then upper limbs, and the rest of the body.
This weakness is rapidly progressive, and in severe cases, clients may develop difficulty moving, walking, or even flaccid paralysis, as well as decreased or absent deep tendon reflexes in the affected limbs.
The cranial nerves can also be involved, causing symptoms like double vision and difficulty speaking. In addition, weakness of the pharyngeal muscles causes difficulty swallowing and increases the risk of aspiration.
In severe cases, nerves supplying the respiratory muscles like the diaphragm can be involved, leading to difficulty breathing and potentially respiratory failure. In addition, when sensory nerves are affected, there’s a loss of sensation, or numbness, and paresthesia, or a feeling of pins and needles, and some clients may even feel pain.
Finally, some clients may experience autonomic dysfunction involving various organs, leading to symptoms like constipation and urinary incontinence, as well as cardiac arrhythmias, fluctuations in blood pressure like hypo- or hypertension, and diaphoresis or increased sweating.
Typically, symptoms of Guillain-Barré syndrome tend to get worse over the next days to weeks, and then start to improve. Most clients completely recover, usually in 4 months to 2 years, as the myelin regenerates. Unfortunately, some clients may retain permanent sequelae, and a minority of cases may result in death from acute complications, such as respiratory failure or infection, as well as pulmonary embolism, and cardiac arrest.
Diagnosis of Guillain-Barré syndrome starts with history and physical assessment, followed by a lumbar puncture to obtain cerebrospinal fluid or CSF. The CSF typically shows an albuminocytologic dissociation, which means that there’s an increase in protein or albumin levels, without an increase in white blood cells. In addition, nerve conduction tests and electromyographic studies can be done to assess nerve and muscle function, but sometimes these tests can be normal early on in the disease. In addition, pulmonary function tests can be done to evaluate an individual’s respiratory function.
Treatment of Guillain-Barré syndrome is aimed at reducing the symptoms, and involves medications that suppress the immune system, such as corticosteroids. Some clients can also be treated with intravenous immune globulins or IVIGs, in order to quickly neutralize the troublesome antibodies; or with plasmapheresis, or plasma exchange to filter out the circulating antibodies from the client’s blood. Finally, clients are also monitored closely for any sign of respiratory failure and they are provided with ventilatory support in case of breathing difficulties, as well as hemodynamic support as needed.