Herpes simplex virus (HSV): Nursing
Herpes simplex virus (HSV): Nursing
2144 final exam
2144 final exam
Notes
| HERPES SIMPLEX VIRUS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
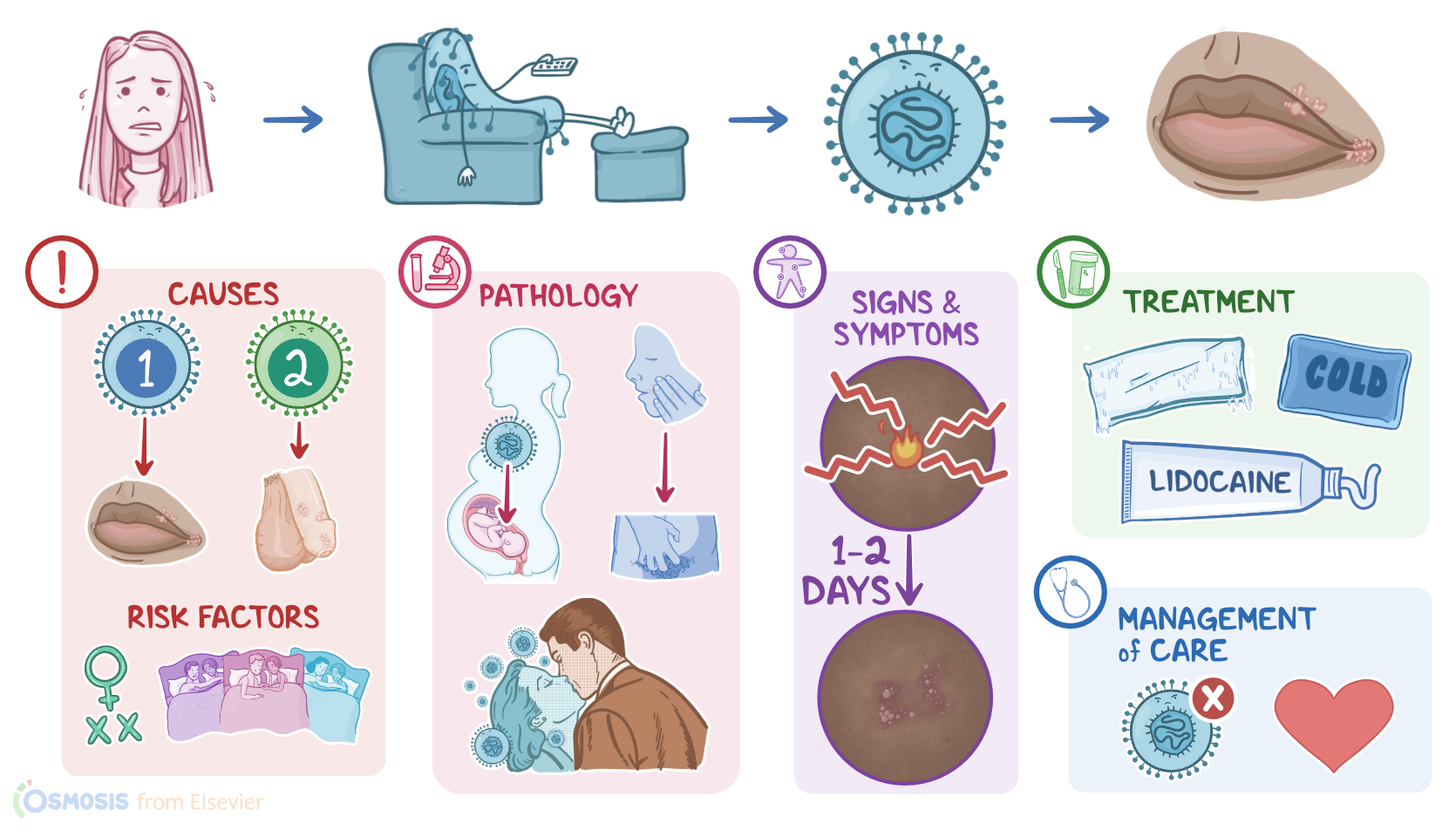
Herpes simplex is a highly contagious infection caused by herpes simplex viruses. There are two types of herpes simplex virus. Herpes simplex virus 1, HSV-1, tends to cause infections above the waist, typically affects the lips, and that’s called herpes labialis; while HSV-2 tends to cause infections below the waist, involving the genitals, and that’s herpes genitalis.
During the primary infection, both types also infect nearby sensory neurons and travel up their axon to sensory ganglia where they can lay dormant for life causing recurrent infections from time to time.
Okay first, let’s quickly review the physiology of the nervous system. The central nervous system consists of the brain and spinal cord, while the peripheral nervous system includes all the nerves that connect the central nervous system to the skin, muscles, and other organs.
Cranial nerves are peripheral nerves that originate from the brain, and they’re mostly in charge of motor and sensory innervation of the head and neck.
A specific cranial nerve, cranial nerve V, is the trigeminal nerve and it’s responsible for the sensation in the face. Its sensory neurons create a nerve cell cluster called the trigeminal ganglion, located in the bones on the side of the face between the eyes and ears.
On the flip side, the peripheral nerves that originate from the spinal cord are called the spinal nerves.
Each nerve is formed by a dorsal root that contains sensory information, like touch, temperature, pain, and pressure from the skin and other tissues, and a ventral root that contains neurons that carry motor innervation from the spinal cord to the muscles.
Alright now, an important risk factor associated with both types of herpes simplex is having multiple sexual partners.
Additionally, specific risk factors for HSV-1 include coming in contact with another person’s saliva, most commonly through kissing or sharing drinks; playing contact sports, like wrestling; and sharing cosmetics.
On the flip side, risk factors for HSV-2 infection include being assigned female at birth and having unprotected sex.
Now, moving on to pathology. Herpes simplex viruses are highly contagious, and they are usually spread through direct contact with herpetic lesions, saliva, or genital secretions of symptomatic or asymptomatic individuals.
Another way of viral spreading is called autoinoculation, which occurs when an infected person spreads the virus from the affected part of their body to an unaffected body part.
Finally, HSV can also pass from a mother to a baby, most commonly when the baby passes through an infected genital tract during delivery.
Okay, now when the virus reaches a new host, it uses small cracks in the skin or mucosa to enter the body. Once inside the epithelial cells, the virus starts to replicate, eventually forming new viral particles that go on to infect neighboring epithelial cells.
This is called primary infection. Next, the virus infects sensory neurons of the skin and travels to their cell bodies which are found in ganglia where it settles for life. Specifically, in genital herpes, the virus lives in the sacral ganglia; while in herpes labialis, the virus lives in the trigeminal ganglion.
In the ganglia, the virus remains dormant, but in times of stress, infections, or immunosuppression, it can start to replicate again, and newly formed viruses use the axon to reach epithelial cells and infect them. This condition is called recurrent infection.
Since the trigeminal and sacral ganglions collect sensory information only from one side of the face and body, herpes vesicles and ulcers develop on the same side as the affected ganglion.
Now, clinical manifestations of primary HSV infection can be totally absent. But, some clients might develop burning and itching at the site of inoculation, followed by the appearance of small, tender, fluid-filled blisters that eventually progress to ulcers and crusts. The lesions typically last from 2 to 6 weeks and heal without scarring. Other features may include flu-like symptoms, like fever, malaise, sore throat; regional lymphadenopathy.
Similarly, in most cases of recurrent herpes simplex, there are no symptoms at all. But, when symptoms do occur, they usually start with a prodromal period, which is associated with burning and tingling sensation in the area that is affected. After one to two days, herpetic lesions appear and they are usually less severe when compared to the primary infection.
Now, regarding the site of the infection, HSV-1 usually affects the lips and causes herpes labialis or cold sores; but it can also infect the skin, gingiva, and mouth causing gingivostomatitis.
On the flip side, HSV-2 typically affects the genital region and causes genital herpes; but it can also spread and infect the anal and perineal regions. It’s important to note that even though they tend to infect a specific part of the body, both types of viruses can affect both the mouth and the genitals.
Herpes simplex viruses can also affect other parts of the body. For example, herpetic whitlow is an HSV infection that appears on the fingertips or nail beds; herpes gladiatorum is an HSV infection of the trunk, extremities, or head; while HSV keratoconjunctivitis is an HSV infection involving the cornea and conjunctiva of the eye.
Herpes simplex rarely causes complications, but if they do occur, they can be serious. HSV-1 can affect the central nervous system and cause encephalitis that most commonly affects the temporal lobes and can present with altered mental status and seizures, while HSV-2 most commonly causes viral meningitis.