Infectious mononucleosis: Nursing
Notes
| INFECTIOUS MONONUCLEOSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
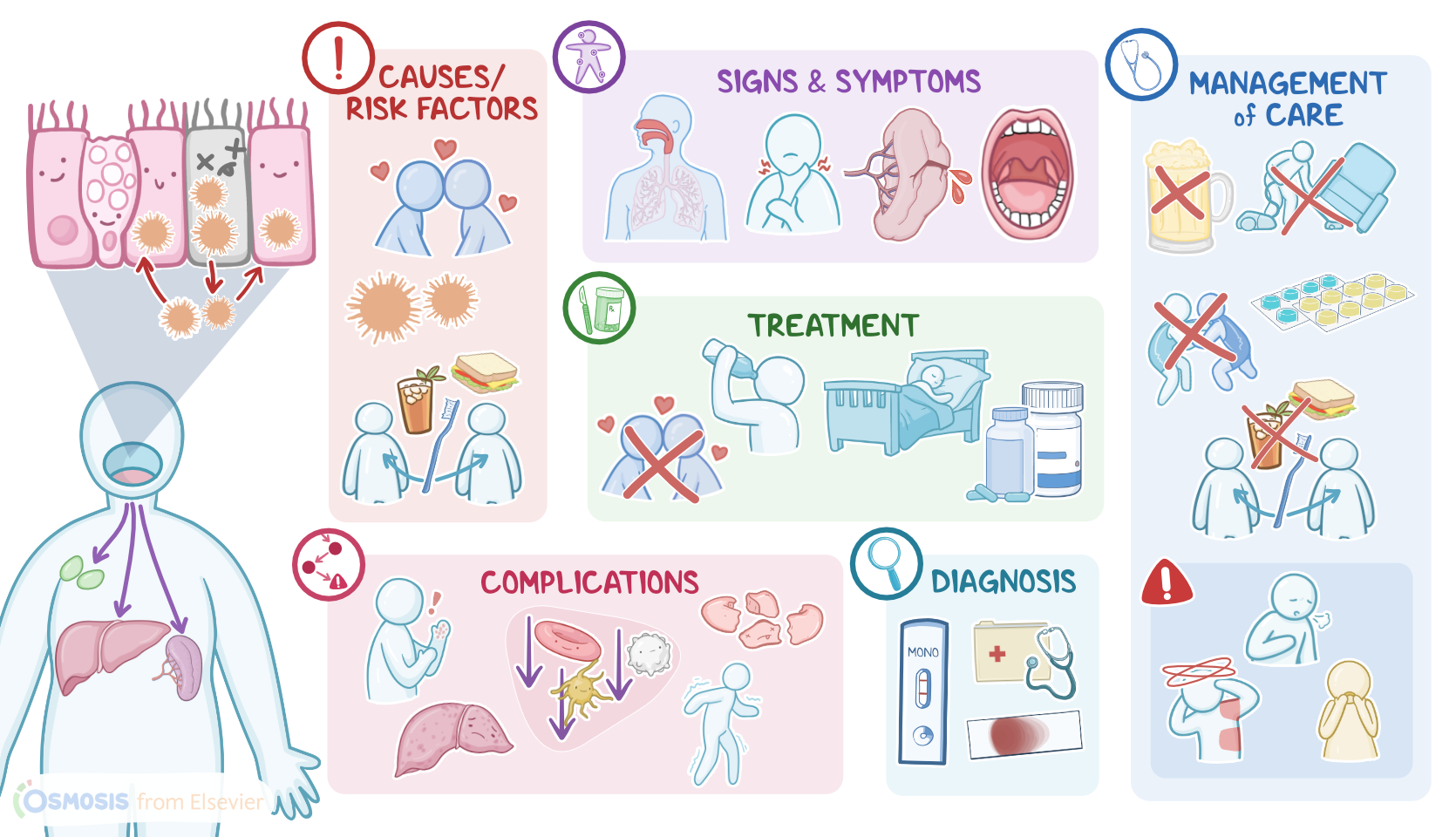
Infectious mononucleosis, or simply mono, is a highly contagious, but self-limiting viral infection caused by the Epstein-Barr virus. Infectious mononucleosis is typically seen in young clients and adolescents and is often referred to as “the kissing disease” because the Epstein-Barr virus primarily spreads through saliva.
First, let’s quickly review the physiology of normal immune response, which is subdivided into innate and adaptive immunity. Innate immunity consists of natural barriers, like skin and mucous membranes; natural killer cells, which help fight virus-infected and tumor cells; and phagocytes, such as macrophages, neutrophils, and dendritic cells.
Now, when a pathogen, like a virus, reaches a person’s mouth, breaches the mucosal barrier, and enters the body, the innate immune system reacts quickly. The first cells on the scene are macrophages and neutrophils, which directly fight the pathogen. At the same time, they also secrete small molecules called cytokines to increase the permeability of local blood vessels and message other immune cells that there’s an active fight in the body. Additionally, cytokines induce the production of acute inflammatory proteins and cause systemic effects, such as fever.
Simultaneously, dendritic cells engulf and digest the pathogen, eventually presenting small fragments of it on their surface. At this point, the adaptive immune system, which relies on B and T lymphocytes, comes to the rescue. Specifically, T helper cells recognize these fragments and help activate B lymphocytes, primarily in pharyngeal lymph tissue, tonsils, and regional cervical lymph nodes. Once stimulated, B cells start to produce antibodies, which circulate throughout the body and bind to pathogens, eventually enabling cytotoxic T lymphocytes and NK cells to recognize and destroy them.
The most common cause of infectious mononucleosis is the Epstein-Barr virus, also known as human herpesvirus 4 or HHV-4. This is a small DNA virus that belongs to the Herpesviridae family. Important risk factors associated with Epstein-Barr infection include kissing, sharing drinks and food, as well as utensils or personal items, like toothbrushes.
Now, let’s look at the pathology of infectious mononucleosis, which starts when the virus-containing saliva or respiratory secretions reach the mouth of a healthy person. Once inside the mouth, the Epstein-Barr virus infects the epithelial cells of the pharynx and starts replicating, eventually forming new viral particles. At one point, newly formed viral particles destroy the host’s cell, eventually spreading the infection and reaching the lymphoid tissue of the pharynx, tonsils, and cervical lymph nodes. Here, the virus infects B lymphocytes. But the Epstein-Barr virus does not kill the B lymphocyte; instead, it enters the latent phase and uses the lymphocyte as a vehicle to spread throughout the body. Eventually, the virus reaches distant sites and causes enlargement of lymph nodes, liver, and spleen, which are conditions also known as lymphadenopathy, hepatomegaly, and splenomegaly, respectively.
Okay, now, important complications that may occur in clients with infectious mononucleosis include erythema multiforme, pancytopenia, and autoimmune hemolytic anemia. Mild hepatocellular hepatitis is also a potential complication. Neurologic complications, such as Guillain-Barre syndrome and aseptic meningitis can also occur. In severe cases, the enlargement of lymph nodes can eventually lead to upper airway obstruction; a peritonsillar abscess can also cause respiratory compromise and dysphagia; while an enlarged spleen can rupture and cause life-threatening bleeding.
Clinical manifestations typically occur 4 to 8 weeks after the infection. First, there can be a prodromal period that includes a gradual onset of fever, chills, malaise, and anorexia. This is followed by the classical triad of symptoms of continued fever, tonsillar pharyngitis, and lymphadenopathy. In severe cases, cervical lymphadenopathy can lead to upper respiratory airway obstruction. Clients also present with nonspecific symptoms, such as headache and fatigue, which can persist even 6 months after the infection. Other important clinical features include palatal petechiae, or red spots on the palate, and tonsillitis that can involve whitish exudates.
Diagnosis of infectious mononucleosis is based on the client’s history, and physical assessment, followed by a peripheral blood smear, which typically reveals lymphocytosis and elevated aminotransferases. Another important diagnostic method is the Monospot test, which can detect the presence of heterophile antibodies. It’s important to note though the Monospot test can be negative during the first 7 to 10 days of the infection.