Juvenile idiopathic arthritis: Nursing
Notes
| JUVENILE IDIOPATHIC ARTHRITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
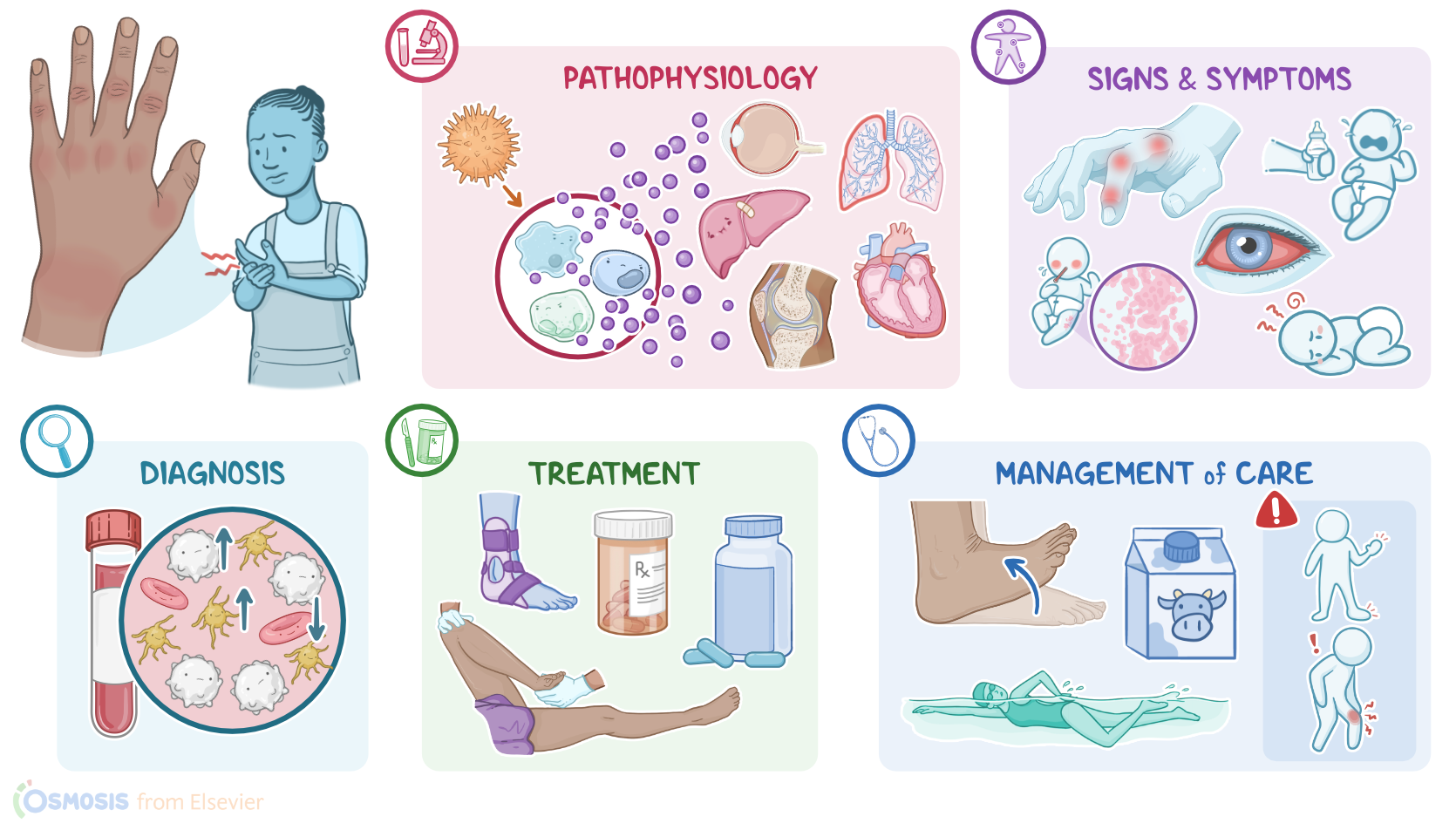
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Juvenile idiopathic arthritis, previously known as juvenile rheumatoid arthritis, is an inflammatory disease that occurs in children and young adolescents under the age of 16.
Alright first, let’s start by reviewing some immune system physiology. So when an antigen enters the body, it comes in contact with a type of immune cells called antigen presenting cells, or APCs. These include macrophages, dendritic cells, and even naive B cells. The APCs will engulf and digest the pathogen then present fragments on their surface. Another type of immune cells, called T helper cells, then recognize the antigen, causing them to activate and proliferate; this results in an army of T helper cells that release cytokines, including interleukin 1, interleukin 6, and tumor necrosis factor, or TNF for short. These cytokines are signalling molecules that attract other immune cells to the site. These cells can be part of the adaptive immune system, like cytotoxic T cells, or killer T cells; or part of the innate immune system, like neutrophils and natural killer, or NK cells. In addition, T helper cells can also trigger another type of immune cells called B cells to secrete antibodies against the antigen.
Finally, after the immune response ends, some immune cells, called memory cells, survive and can remember an antigen, allowing them to activate a quicker immune response to that antigen in the future.
Okay, as the term idiopathic suggests, the exact cause of juvenile idiopathic arthritis is unknown. However, several risk factors have been identified. These include genetic factors, like having a particular HLA subtype called HLA-B27; being assigned female at birth; as well as antibiotic use during infancy and childhood. On the bright side, some possible protective factors have also been identified, including having been breastfed.
Now, while the exact mechanism of the disease is unknown, it is believed that an environmental factor triggers an atypical autoimmune response in genetically susceptible individuals. There could be an imbalance of immune cells with less regulatory cells to slow down the immune response and distinguish self from non-self molecules and more T-helper cells, or innate immunity cells, like macrophages and neutrophils, and proinflammatory cytokines. This imbalance promotes inflammation.
Additionally, autoantibodies, meaning antibodies that target self-molecules, are produced and target various structures in joints. As inflammation increases, the joints as well as other organs can become damaged, and eventually arthritis may occur.
Now, there are three types of juvenile idiopathic arthritis. The most common type is oligoarticular, also called pauciarticular, in which there are up to 4 joints affected. Then, there is polyarticular which involves five or more joints, most commonly small joints, affected symmetrically, similar to rheumatoid arthritis in adults. These two types can also be associated with uveitis, which is an inflammation in the middle layer of the eye, as well as with enthesitis, where tendons are also involved.
Finally, there is systemic juvenile arthritis which affects not only the joints but also various other tissues throughout the body. These include pericarditis, meaning inflammation of the pericardium, which is the fibrous sac that surrounds the heart; and pericardial effusion, which is a fluid buildup in the pericardial cavity. Similarly, systemic arthritis can also cause pleuritis, or the inflammation of the pleura that surrounds the lungs; and pulmonary fibrosis, which is when the healthy lung tissue is replaced with scar tissue. Finally, a serious complication of systemic arthritis is macrophage activation syndrome, which is when there is an overproduction of macrophages and T cells. These cells can infiltrate many tissues in the body, like the liver, spleen and lymph nodes, causing them to enlarge.
Alright now, juvenile idiopathic arthritis presents with typical inflammatory joint signs, such as pain, redness, warmth, swelling, and stiffness of the joints. These are more pronounced after inactivity, like when waking up in the morning. Symptoms improve with movement. In very young children, irritability and fussiness can be early signs.
Now individuals with juvenile idiopathic arthritis may also experience malaise and poor appetite. They can also have lymphadenopathy and organomegaly, including enlargement of the spleen and liver. Additionally, if uveitis is present, individuals can present with red eyes, pain, photophobia and blurred vision.
Finally, in systemic arthritis, the skin can be affected too, mainly showing a salmon pink macular rash that often appears with fever. Other systemic abnormalities that can occur include a spiking fever, pericarditis and pleuritis.
The diagnosis of juvenile idiopathic arthritis is mostly clinical and it is based on the client's history and physical assessment. Laboratory tests can also be ordered, and typical findings can include a mild to moderate anemia; leukocytosis, especially T cells; and thrombocytosis; as well as increased erythrocyte sedimentation rate, or ESR, and C-reactive protein, or CRP. Individuals with juvenile idiopathic arthritis can also be positive for antinuclear antibodies, or ANA, rheumatoid factor, or RF, while genetic testing might be positive for HLA-B27. The final step in the diagnostic process is imaging of the joints, typically an X-ray first, followed by an ultrasound or MRI.
Now, there is no cure for juvenile idiopathic arthritis, so treatment is supportive. The treatment focuses on controlling inflammation, relieving pain, promoting remission, maintaining mobility, minimizing deformity, and reducing the impact on growth and development. To reduce inflammation and pain, initially, non-steroidal anti-inflammatory drugs, or NSAIDs, are used. When their effectiveness wanes, corticosteroids or other immunosuppressant medications are prescribed. Methotrexate is often the first choice while in more severe polyarticular disease, anti-TNF factors like etanercept are used.