Kawasaki disease: Nursing
Kawasaki disease: Nursing
Medical Surgical
Medical Surgical
Notes
| KAWASAKI DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Contributors
Kawasaki disease is a condition associated with acute inflammation of medium-sized arteries; and it’s typically seen in children between the ages of 6 months and 5 years.
First, let’s cover some basic physiology of arteries. There are three main types of arteries: large arteries, like the aorta; medium arteries, like the coronary arteries that supply the heart; and finally, small arteries.
Now, each artery consists of three layers: from outside in, there’s the tunica adventitia, which has loose connective tissue; then the tunica media, which mainly contains smooth muscle cells but also some elastic tissue; and finally the tunica intima, or endothelium, which consists of a single layer of endothelial cells on top of a layer of connective tissue, called lamina propria.
The exact cause of Kawasaki disease remains unknown, but some sources suggest that it might be triggered by an infection or autoimmune process. The most important risk factors associated with Kawasaki disease include being below 5 years of age, being assigned male at birth, and having Asian or Pacific Islander ancestry.
Now let’s look at the pathology of Kawasaki disease. Typically the client’s immune system is activated to fight off an infection. Then, for reasons we still don’t understand, the immune cells like neutrophils, macrophages and even B cells and T cells start attacking the endothelial lining of medium sized blood vessels, most commonly the coronary arteries of the heart. Now, these cells cause inflammation within the artery which damages the endothelial lining. They can even invade into the tunica media where they destroy the elastin and collagen fibers that make up the arterial wall.
Now, Kawasaki disease can cause serious life-threatening cardiovascular complications. First, damage to the endothelium exposes collagen and tissue factors in the tunica media, which can trigger coagulation. Clots forming on the arterial wall reduce blood flow to heart tissue, causing ischemia. Next, inflammation leads to fibrosis within the arterial wall, which makes the walls thicker and the arterial lumen narrower, reducing blood flow even more. Finally, damage to the arterial wall weakens it, so it can balloon out forming an aneurysm. If the aneurysm ruptures, blood flow will be further reduced. So all three processes reduce blood flow to the heart; this causes ischemia, and potentially myocardial infarction or even death.
In addition, the immune cells causing arterial inflammation can move beyond the arterial wall into nearby cardiac tissue causing valvulitis, meaning inflammation of the heart valves; myocarditis, or inflammation of the heart muscle; and pericarditis, or inflammation of the fibrous heart sac called the pericardium.
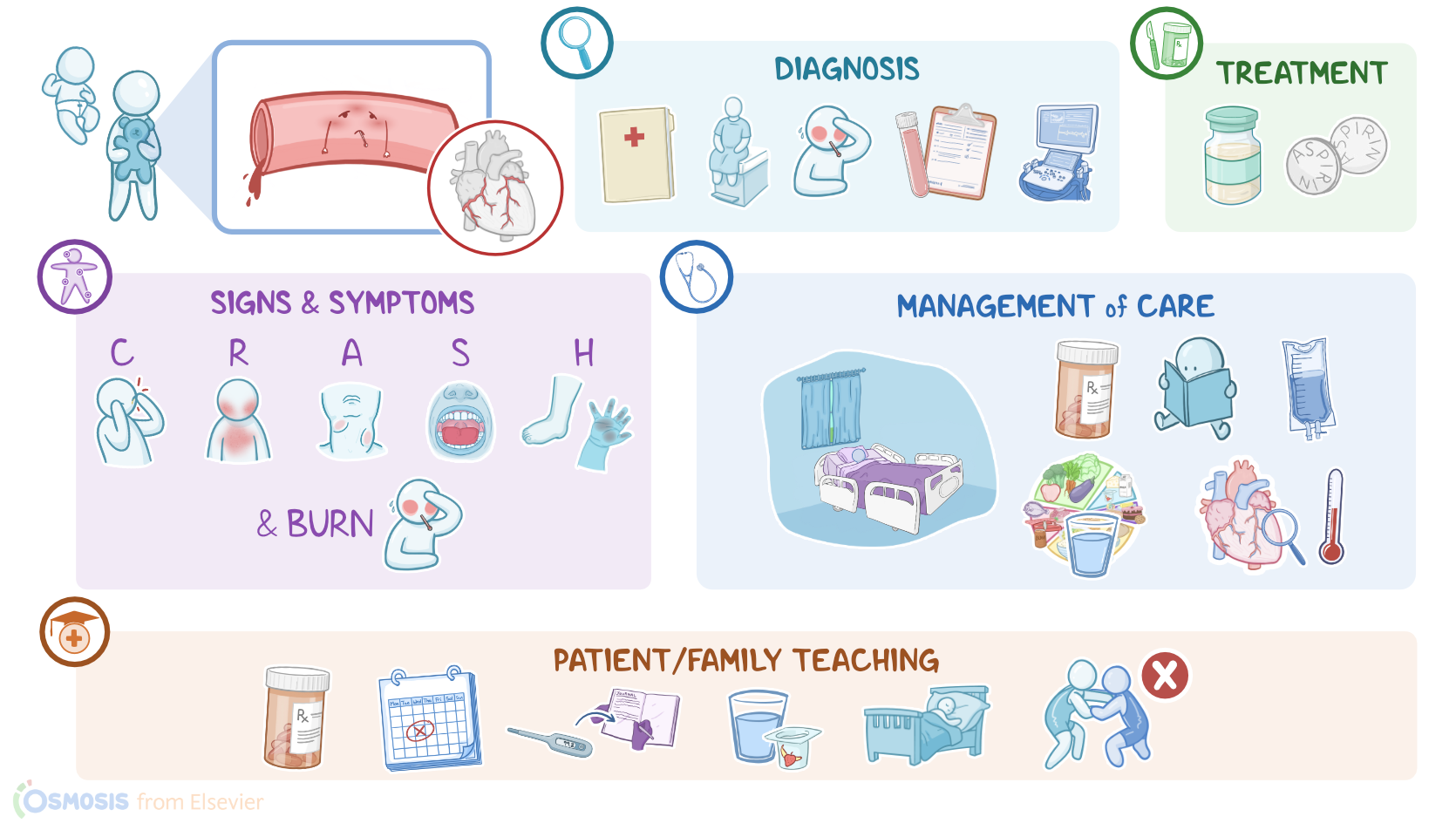
Now, the most important clinical manifestations of Kawasaki disease can be remembered with the mnemonic CRASH and burn. “C” stands for Conjunctival hyperemia or eye redness that can be associated with photophobia, meaning increased sensitivity of the eyes to light. Next, there is “R” for Rash, described as polymorphous exanthem; while “A” stands for Adenopathy, more specifically lymphadenopathy of cervical lymph nodes.
Next up is “S” for Strawberry tongue, which refers to a red tongue that can be associated with dry and cracking lips. Finally, there’s “H” for Hand and foot changes, which include edema, erythema, as well as desquamation of the skin on tips of fingers and toes; and finally, burn refers to fever. Other clinical manifestations include malaise, joint pain, diarrhea, thrombocytosis, and cardiac manifestations such as cardiac arrhythmias.
Diagnosis is based on medical history and physical examination. A client must have a fever that lasts for over 5 days and at least four of the five clinical features of Kawasaki disease. Additional diagnostic methods that can help include CBC, CRP, ESR, serum transaminase levels, as well as echocardiography, to assess degree of cardiac involvement.
Treatment includes supportive care and minimization of the risk of the coronary aneurysm. Clients should receive intravenous immunoglobulin, as well as high-dose aspirin, to prevent thrombosis. Normally, aspirin should be avoided in children because it can cause Reye syndrome, which is a condition characterized by liver failure and rapidly progressive encephalopathy; however, with Kawasaki disease, aspirin is permitted because its anti-thrombotic effects outweigh the risk of Reye syndrome.
All right, let’s take a look at the nursing care you’ll be providing for a child with Kawasaki disease. Your priority nursing goals are to promote comfort and healing, and to monitor for complications.
Start by assisting your client into a position of comfort and create a calm environment by decreasing external stimulation. Also dim the lights in their room to ease the photophobia and discomfort caused by their conjunctivitis. Apply lip balm to their chapped lips and a mild lubricant to areas of rash and peeling skin.