Lymphoma - Hodgkin and non-Hodgkin: Nursing
Lymphoma - Hodgkin and non-Hodgkin: Nursing
223 Content
223 Content
Notes
| LYMPHOMA - HODGKIN AND NON-HODGKIN | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
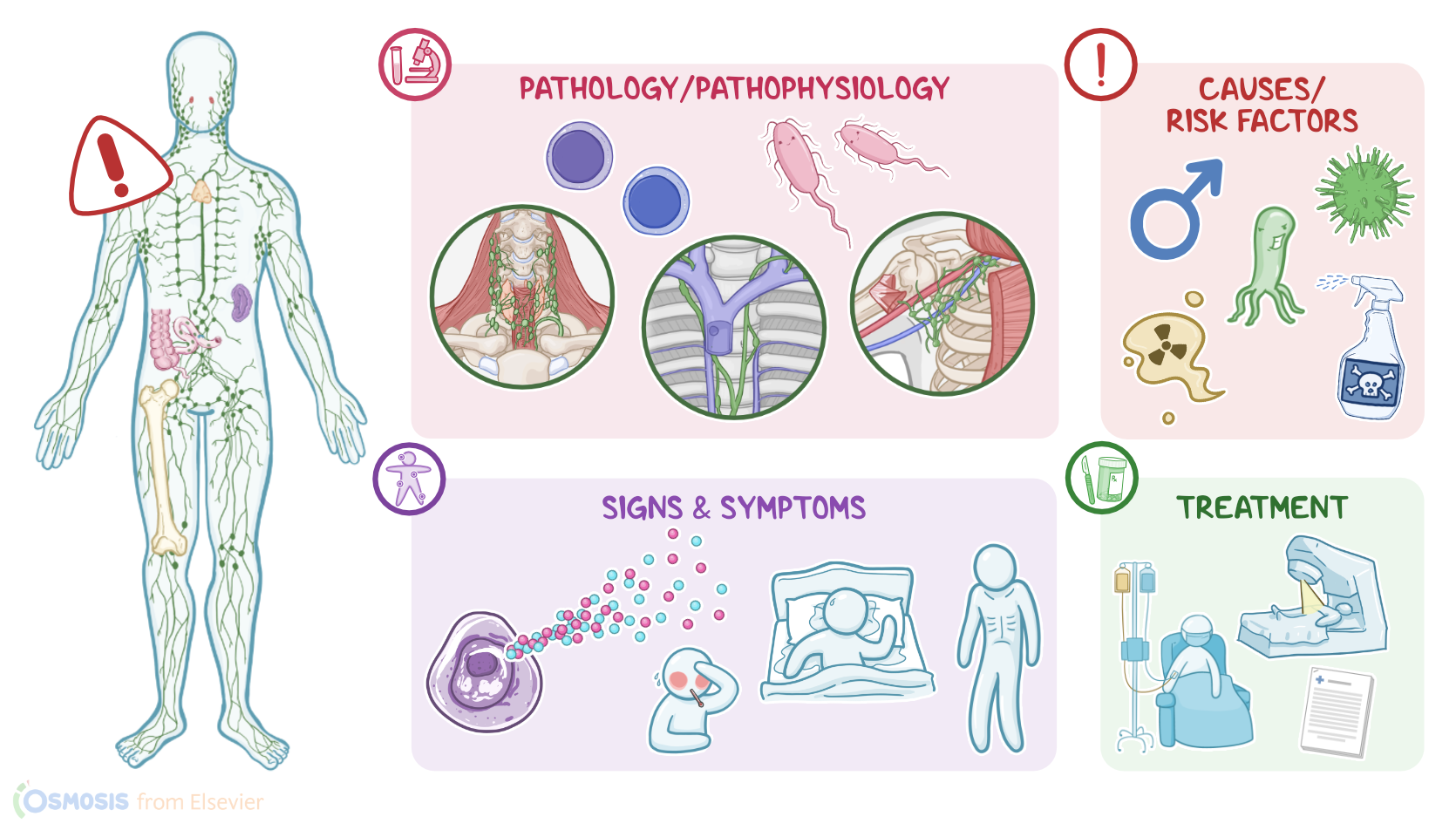
Lymphoma is a tumor derived from lymphocytes, specifically B-cells and T-cells, which are white blood cells that mainly live in lymph nodes and move through the blood and the lymphatic system. Lymphomas can be broadly grouped into two categories; Hodgkin and non-Hodgkin lymphomas. Hodgkin lymphomas tend to spread in a contiguous manner, meaning they spread to nearby lymph nodes, but rarely involve extranodal sites. In contrast, non-Hodgkin lymphomas can sometimes spread non-contiguously, and can involve extranodal sites like the skin, gastrointestinal tract, and brain.
Now, let’s quickly review the anatomy and physiology of the lymphatic system. The lymphatic system protects the body from invaders, maintains the fluid level in the body, and absorbs dietary fat from the intestine. It is composed of lymph, lymphocytes, lymphatic vessels and plexuses, lymph nodes, and other lymphoid organs, such as the thymus, the bone marrow, the spleen, and the tonsils. The lymph is a clear, or slightly yellow, fluid that is transported through tubes similar to blood vessels, called lymphatic vessels. Lymphatic vessels drain lymph through lymph nodes and eventually into lymphatic trunks, which drain large regions of the body, like the subclavian trunks that drain the upper limbs.
Lymphatic trunks converge to form two bigger channels called lymphatic ducts, specifically the right lymphatic duct and the thoracic duct. Now, as lymph travels through lymphatic vessels, it encounters lymph nodes which filter the lymph and check to see if there are any foreign invaders the body needs to attack. In the case of an invader, the lymphocytes react and initiate an immune response. Typically, lymph nodes lie close to each other, forming groups that may lie superficial or deep within the body, such as the cervical lymph nodes, the mediastinal lymph nodes, and the axillary lymph nodes.
Although the exact cause of lymphoma remains unknown, several risk factors have been established. For Hodgkin lymphoma, non-modifiable factors include being assigned male at birth, age between 15 and 30 or over 55, and certain genetic mutations. On the other hand, modifiable risk factors include exposure to viruses, such as Epstein-Barr virus or EBV, a history of autoimmune disorders, and immunosuppression.
Switching gears, for Non-Hodgkin lymphoma, modifiable risk factors include viral infections, like EBV, Hepatitis C, and human T-cell leukemia virus, or HTLV infection, as well as bacterial infections such as Helicobacter pylori. Other risk factors include a history of autoimmune disorders, the use of certain medications, such as immunosuppressants, chemotherapy, and exposure to radiation or toxins, like pesticides.
Alright, now regarding the pathology of lymphoma, there is usually a genetic mutation in a lymphocyte. When something like that happens, cells are supposed to undergo apoptosis or programmed cell death, but instead, the lymphocyte becomes neoplastic, so it starts to divide uncontrollably. Usually, lymphomas develop in lymph nodes and they’re called nodal lymphomas. Lymphomas can happen anywhere in the body, though, and when they develop in other tissues or organs, like the stomach or skin, they’re called extranodal lymphomas. Lymphoma cells can also get into the blood and can spread to other parts of the body, such as the gastrointestinal tract, the bone marrow, or the spinal cord.
Okay, now Hodgkin lymphoma, typically arises from B-cells and tends to spread in a contiguous manner, meaning it spreads to nearby lymph nodes, and rarely involves extranodal sites. Neoplastic cells are large mononuclear cells called Hodgkin cells, or multinucleated cells called Reed-Sternberg cells. Classically the Reed-Sternberg cells are two cells that are fused together, forming a large cell with two nuclei, which looks like owl eyes. There are also two major types of Hodgkin lymphoma, classical Hodgkin lymphoma, and nodular lymphocyte-predominant Hodgkin lymphoma. According to histologic features, classical Hodgkin lymphoma can be further subdivided into four subtypes: nodular sclerosis, mixed cellularity, lymphocyte-rich, and lymphocyte-depleted Hodgkin lymphoma.
Non-Hodgkin lymphomas often spread non-contiguously, can involve extranodal sites like the skin, gastrointestinal tract, and the brain, and don’t contain Reed-Sternberg cells. Non-Hodgkin lymphomas can originate from B cells or T cells, though they most commonly arise from B cells. Diffuse large B-cell lymphoma is the most common type of non-Hodgkin lymphoma among adults, while the most aggressive one is Burkitt lymphoma. Follicular lymphoma, on the other hand, is the most common indolent or slow-growing non-Hodgkin lymphoma. Common T-cell lymphomas include adult T-cell lymphoma and mycosis fungoides.
As far as clinical manifestations go, clients with lymphoma usually develop painless lymphadenopathy. The release of cytokines by lymphoma cells can also cause a characteristic triad of symptoms including fever, drenching night sweats, and unintentional weight loss, known as B symptoms. If there’s extranodal involvement of the gastrointestinal tract, it can cause crampy abdominal pain due to bowel obstruction. If there’s extranodal involvement of the bone marrow, it can cause fatigue due to decreased red blood cells, easy bruising due to low platelets, or recurrent infections due to decreased white blood cells. And if there’s extranodal involvement of the spinal cord, it can cause weakness and a loss of sensation, usually in the legs. On physical assessment, an enlarged liver or spleen might be palpated.
Diagnosis of lymphoma starts with the client's history, and physical assessment, followed by lymph node biopsy to confirm the diagnosis and determine whether it’s Hodgkin or Non-Hodgkin lymphoma based on the presence of Reed-Sternberg cells. Additional tests, like a CT scan, a PET scan, or a bone marrow biopsy, are typically done to stage the lymphoma, based on the extent of nodal and extranodal involvement.
The treatment of lymphoma depends mostly on the lymphoma type, and stage, as well as other factors like the age and general health of the client and other conditions they may have. Treatment options include chemotherapy, radiation therapy, targeted therapies, like imatinib, but also novel therapies like chimeric antigen receptor, or CAR T-cell therapy. Overall, the prognosis for Hodgkin lymphoma is better than that of non-Hodgkin lymphoma.
Alright, let’s look at the nursing care you’ll be providing for a client receiving chemotherapy for non-Hodgkin lymphoma. Your priority nursing goals are to manage complications related to the treatment regimen and to provide psychosocial support.
Now, before starting chemotherapy, administer the prescribed antiemetics to help prevent nausea and vomiting related to chemotherapy. Then, implement measures to reduce the risk of tumor lysis syndrome or TLS, which can occur during chemotherapy as potassium, phosphorus, and nucleic acids from dying cancer cells spill into the bloodstream. First, ensure your client is well hydrated and that their urine output amounts to about 3 L/day; this will decrease the risk of acute kidney injury from uric acid and calcium phosphate deposits in the renal tubules. Also be sure to monitor for fluid overload and pulmonary edema during this time; and administer the prescribed allopurinol to help prevent hyperuricemia.
Then, as you administer the prescribed chemotherapeutic medications, keep a close eye on your client’s response to the treatment, as well as their most recent laboratory test results. Stop the chemotherapy infusion and immediately report to the healthcare provider if your client’s laboratory report shows hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, and increased serum creatinine; or if they experience clinical manifestations of TLS such as oliguria, cardiac arrhythmias, or seizure activity.
Then, begin lowering the serum potassium by administering the prescribed IV 50% dextrose and short-acting insulin; and IV calcium gluconate to stabilize the cardiac conduction and replenish calcium stores. To lower phosphate levels, continue IV fluids and administer a phosphate binder. Lastly, administer a recombinant urate oxidase medication to treat hyperuricemia.