Methicillin-resistant Staphylococcus aureus (MRSA): Nursing process (ADPIE)
Methicillin-resistant Staphylococcus aureus (MRSA): Nursing process (ADPIE)
Exam 1 Playlist Spring 2025 Pathophysiology: Haber & Vela
Exam 1 Playlist Spring 2025 Pathophysiology: Haber & Vela
Notes
| METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
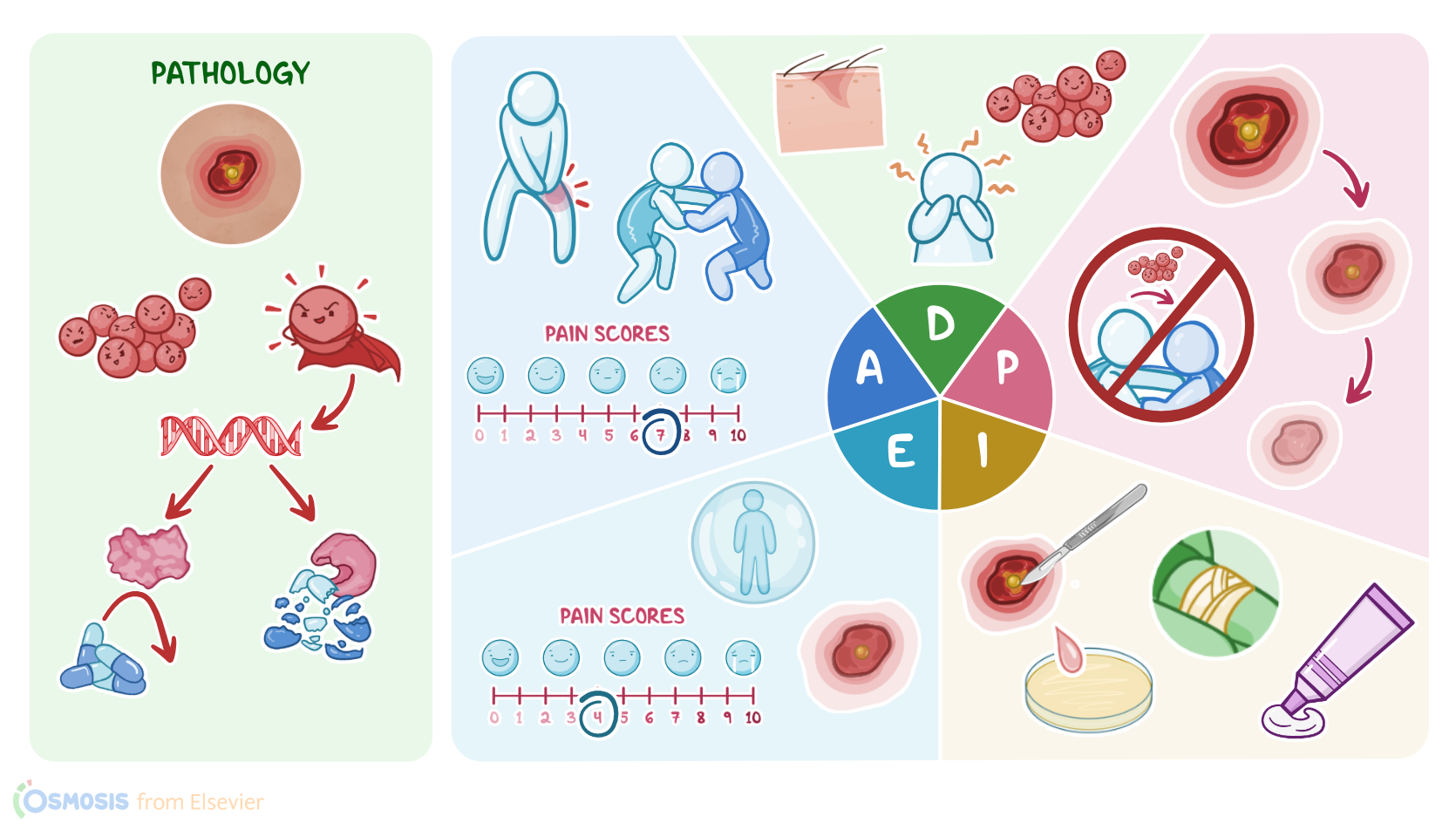
Elias Moore, a 17-year-old African American male, who is on his school’s wrestling team who developed a red, painful sore on the upper left side of his thigh.
At first it looked like a spider bite, but the next day it began to swell and formed a bump filled with pus.
He showed it to his mother who took him to the pediatrician’s office where he was diagnosed with community-acquired methicillin-resistant Staphylococcus aureus, also known as CA-MRSA.
MRSA is a strain of Staphylococcus aureus, or staph for short.
It’s often referred to as a superbug due to its resistance to the widely-used beta lactam antibiotics such as penicillins, cephalosporins, and carbapenems.
This is because MRSA has the mecA gene that allows the bacteria to produce proteins that are more difficult for the medications to bind to, and it also codes for the beta lactamase enzyme which can break these medications down.
Unfortunately, due to the misuse and overuse of antibiotic treatment by both clinicians and patients, MRSA has become more common in recent years.
The two types are healthcare-associated MRSA, or HA-MRSA, and community-associated MRSA, or CA-MRSA.
HA-MRSA infections are a leading cause of infection in hospitals due in part to the fact that it creates biofilms that colonize medical devices like catheters, endotracheal tubing, and surgical instruments.
On the other hand, CA-MRSA occurs when there’s been no exposure to the healthcare setting and it can affect healthy individuals.
CA-MRSA is primarily transmitted from direct or indirect contact and can either asymptomatically colonize or cause an active infection.
Risk factors for developing an active infection include chronic illnesses like kidney disease, diabetes, or malignancies; activities that could cause damage to the skin, like contact sports and intravenous drug use; living in crowded or unsanitary conditions like army barracks or prisons; and those with HIV or using immune suppressing medications like corticosteroids.
The infection occurs when immunosuppression or altered skin integrity allows the bacteria to bypass the body’s natural defenses and enter the tissue.
CA-MRSA typically presents as a localized skin and soft tissue infection, or SSTI.
Single or multiple red bumps that resemble pimples or spider bites initially appear in areas of compromised skin integrity or in areas often covered with hair like the armpits, groin, or back of the neck.
Increased warmth, erythema, edema, tenderness, a palpable fluid-filled cavity, or purulent drainage may occur within the infected site.
Fever and lethargy are also commonly experienced at this time.
If left untreated or poorly managed, these localized infections can quickly become systemic and result in sepsis, endocarditis, osteomyelitis, necrotizing pneumonia, and septic joints.
CA-MRSA can be diagnosed through a variety of tests.
Cultures from suspected sources of infection, such as wound scraping, sputum, blood, or urine, can be collected for testing.
If the culture’s results remain inconclusive, the DNA polymerase chain reaction, or PCR, of MRSA is highly sensitive and currently considered the gold standard for determining infectious type.
To test for MRSA colonization and not active infection, DNA PCR of MRSA from a nares swab is often utilized.
Treatment for MRSA involves quick initiation of antibiotic therapy.
HA-MRSA infections typically have more resistance to medications when compared to CA-MRSA.
In fact it often resists non-beta lactam antibiotics, making it more difficult to treat.
Common oral antibiotics prescribed include trimethoprim/sulfamethoxazole, doxycycline or minocycline, clindamycin, linezolid or tedizolid, and delafloxacin.
Intravenous antibiotics may be initiated if the oral medications prove ineffective, if systemic infection occurs, or if the SSTI occurred near an implanted device.
In such cases, IV vancomycin is often the preferred drug among clinicians.
However, new strains of vancomycin-resistant Staphylococcus aureus, known as VRSA, have become more common in recent years.