Musculoskeletal injuries: Nursing process (ADPIE)
Musculoskeletal injuries: Nursing process (ADPIE)
RNSG 2020
RNSG 2020
Notes
| MUSCULOSKELETAL INJURIES | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
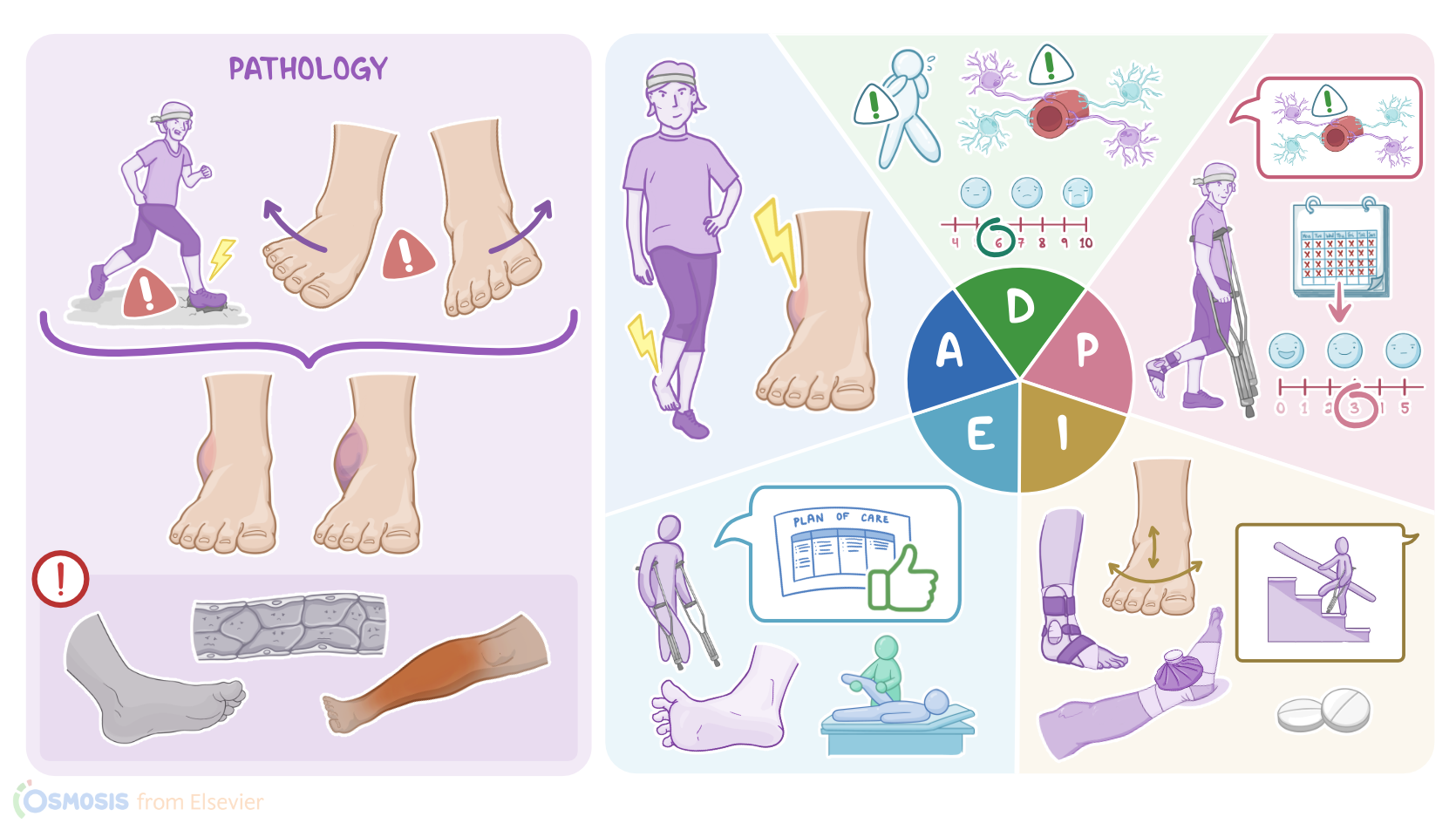
Liam Warner is a 24-year-old male who is dropped off at the urgent care clinic with right ankle pain and swelling. This morning Liam was running in a 10K run when his foot landed on an uneven surface, injuring his ankle. He says “My foot didn’t land right and I could feel it rolling inward. I wasn’t able to finish because I could barely walk.” While in the clinic, an ankle X-ray series rules out a bone fracture, and a grade 2 sprain is suspected.
Local musculoskeletal injuries mainly include conditions that affect bones, joints, muscles, and ligaments. The most common ones include bone fractures; joint dislocations; muscle or tendon strains; and finally, ligament sprains. Now, sprains typically occur when the physical force applied to the joint exceeds the elasticity of the surrounding ligaments. And this is particularly common in ankle injuries, when there’s incorrect positioning of the foot at landing, like when a person is walking or running on an uneven surface; or they fall and twist their ankle; another frequent scenario involves jumping and awkwardly landing on their foot; or being stepped on during a sports game.
Now, there are two main types of ankle sprains. Lateral sprains are the most common ones and they are typically caused by forced inversion of the foot. In other words, a person’s sole rotates inwards or medially, but too much, eventually damaging the ligaments located on the outer side of the joint. On the other hand, medial sprains are caused by forced eversion of the foot, meaning a sole rotates outwards or laterally, eventually damaging the medial ligaments.
Alright, there are some factors that can put a person at risk for ankle sprains. Modifiable risk factors include wearing inappropriate footwear, having poor athletic condition, not warming up before training, and fatigue from overtraining or intense physical activity. On the other hand, non-modifiable risk factors include being male between the ages of 15 to 24, or being female over the age of 30, as well as previous history of ankle sprains; balance problems; and conditions associated with foot misalignment, such as pes cavovarus, often referred to as overarched foot.
Depending on how severe the injury is, ankle sprains can be classified into one of three grades. Grade one ankle sprains refers to mild stretching of the ligament, and it’s typically associated with mild pain and swelling. Grade two ankle sprains involve a partial rupture of the ligaments and present with moderate pain and swelling, as well as bruising. There is mild to moderate joint instability, with some restriction in ankle motion, and both walking and weight bearing are painful. Finally, grade three ankle sprains involve complete ligament tears, and present with severe pain, swelling, and bruising; as well as significant joint instability with loss of function and weight bearing.
Now, most ankle sprains heal without causing any complications. Rarely though, some clients may develop acute complications from associated muscle or blood vessel injuries, such as acute compartment syndrome. This is a serious condition in which there’s a rapid increase in the pressure within an enclosed compartment, leading to tissue damage due to hypoxia and ischemia. On the other hand, long-term complications may occur years after the injury. The most common ones include joint instability or stiffness, as well as osteoarthritis, all of which can ultimately result in impaired range of motion.
In most cases, diagnosis is based on history and physical examination. If a fracture is suspected, it can be confirmed by performing an X-ray. An MRI can be done to evaluate the condition of the surrounding soft tissue or detect a hidden fracture.
Treatment of ankle sprains is usually symptomatic and includes the PRICE method, which stands for protection and rest, by immobilizing the ankle with a brace or controlled ankle motion boot or CAM boot; as well as ice, compression, and elevation of the affected ankle to reduce the swelling. Additionally, below-knee casts can be used to reduce the length of the recovery period; while pain and inflammation can be managed with acetaminophen or NSAIDs like ibuprofen. This is followed by mobilization of the ankle with physical therapy and gradual exercises to recover the full mobility and strength of the ankle. Fortunately, surgery is rarely needed for ankle sprains.
After introducing yourself as his nurse you begin your assessment. Liam’s vital signs are oral temperature 98.2° F or 36.8° C; heart rate 62 beats per minute, respiratory rate 16 breaths per minute, blood pressure 115/70 mmHg, SpO2 100% on room air and pain 6/10. Liam’s right foot and ankle are edematous with ecchymosis on the lateral side of his foot. The ankle is warm and tender to palpation around the lateral malleolus. Capillary refill in less than 3 seconds, he can wiggle his toes, and you palpate strong posterior tibial and dorsalis pedis pulses.
He is able to bear toe-touch weight and take 5 limping steps. Next, you elevate Liam’s ankle above the level of his heart and apply an ice pack. After documenting your assessment findings, you let Liam know the physician assistant, or PA, will be in to examine him shortly.