Neonatal sepsis: Nursing
Notes
| NEONATAL SEPSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Neonatal sepsis refers to the presence of bacteria in the blood or bacterial meningitis presenting in the first 30 days of life. It is classified as early-onset and late-onset sepsis. Early-onset sepsis occurs during the first three days of life, and is caused by exposure to a pathogen during the intrapartum period; while late-onset sepsis occurs after the first week of life, and is caused by pathogens that are acquired postnatally.
Now, let’s quickly review the immune system of newborns. During the first six months of life, the immune system is immature, meaning that it reacts more slowly to an invasion when compared to older children. Because the infant’s immune system isn’t fully developed, they depend on the few antibodies acquired from the mother during the intrauterine life and from breast milk. These offer some protection but are too few to keep infections localized, so there’s a higher risk of infections spreading quickly throughout the body. Additionally, the newborn’s blood-brain barrier is underdeveloped, and that makes it easier for pathogens to enter the central nervous system and cause meningitis.
Now, neonatal sepsis is most commonly caused by bacteria from the mother’s genitourinary tract that infects the infant during delivery. The most common ones include group-B Streptococcus, Streptococcus pyogenes, Escherichia coli, Listeria monocytogenes, Haemophilus influenzae , Enterobacter spp. Less commonly, sepsis can be caused by fungi, such as Candida albicans.
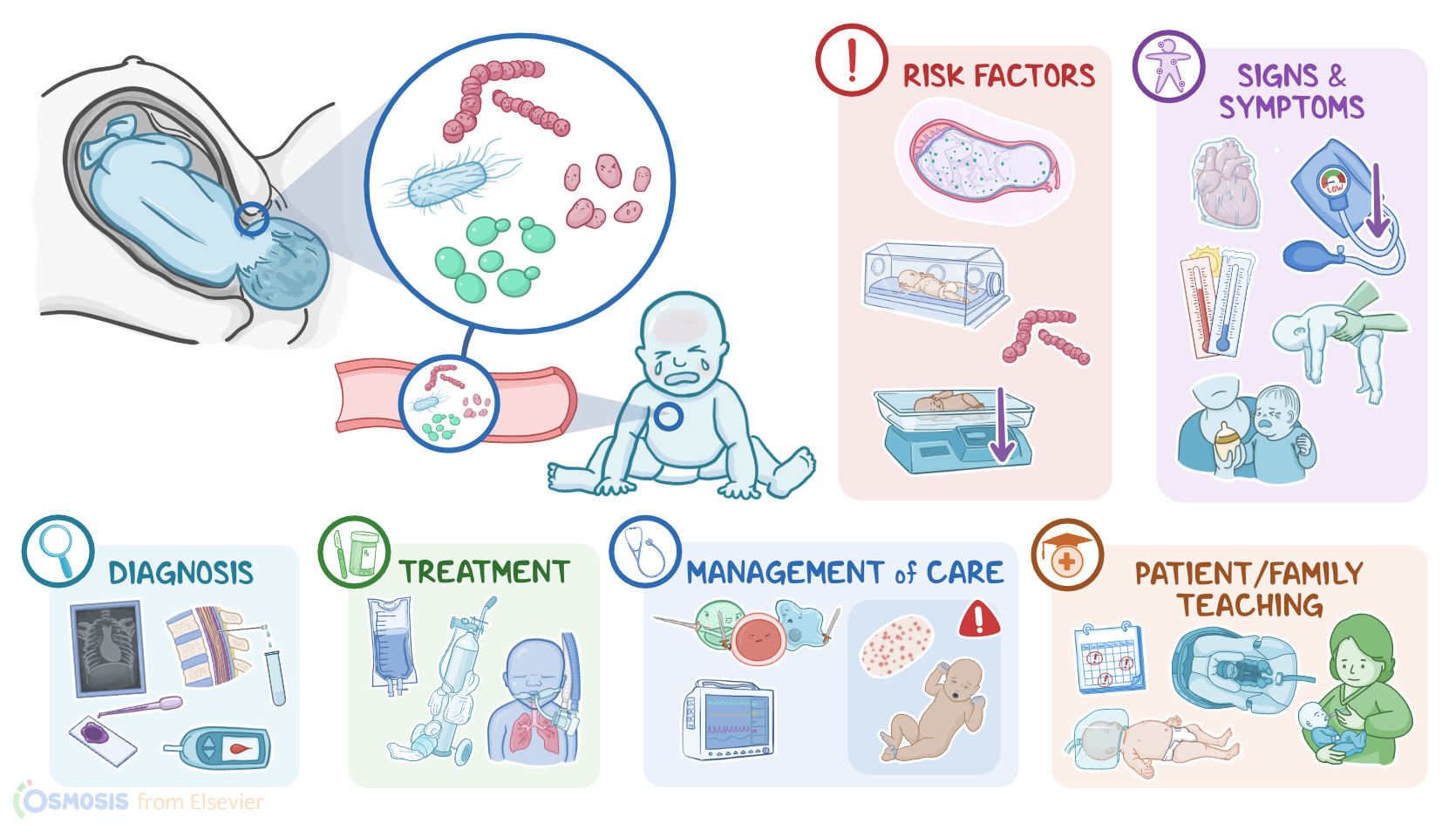
Risk factors for neonatal sepsis are grouped into fetal and maternal risk factors. Fetal risk factors include prematurity, low birth weight, and admission to the neonatal intensive care unit, or NICU for short. On the other hand, maternal risk factors include prolonged rupture of membranes that lasts 12 to 18 hours prior to delivery, in addition to chorioamnionitis, and vaginal colonization by group-B Streptococcus.
Alright, now the pathological process of neonatal sepsis starts when a pathogen, say some bacteria, enters the body. With the immune system still immature and the immunoglobulin levels at a lower level, there’s a higher risk that some bacteria will make it into the bloodstream. At this point, the bacteria and the toxin they release can activate immune cells to release proinflammatory cytokines, which trigger widespread inflammation. These bacteria and toxins can also find their way to various body organs, and cause impaired pulmonary, hepatic, and renal function.
Now, neonatal sepsis can lead to important acute complications, including septic shock, as well as disseminated intravascular coagulation, or DIC for short, and multiple organ dysfunction syndrome, or MODS for short. Neonatal sepsis can also cause long-term complications, such as chronic lung disease, cerebral palsy, impaired psychomotor and mental development, in addition to neurodevelopmental abnormalities, such as hearing and visual deficits.
Before birth, clinical manifestations of neonatal sepsis may include intrapartum fetal tachycardia, nonreassuring fetal heart rate patterns, and meconium stained amniotic fluid.
Clinical manifestations after birth can include an Apgar score of 6 or lower at 5 minutes; lethargy; decreased tone; feeding difficulties, including weak suck, poor feeding, and abdominal distension;
temperature instability; signs of respiratory distress, including tachypnea, nasal flaring, chest retractions, grunting, cyanosis; apnea accompanied by bradycardia; as well as hypotension.
In the case of meningitis, the neonate may also be irritable; have a full or bulging fontanelle; and can present with nuchal rigidity or seizures.
The diagnosis of neonatal sepsis starts with a history and physical examination, followed by cultures of the blood, urine and cerebrospinal fluid to identify the causative organism. Cerebrospinal fluid is also sent for Gram stain, and analysis of the fluid will show an elevated protein level, or low glucose level in the case of bacterial meningitis. In the meantime, a CBC with differential is performed, which typically shows an increased or decreased WBC count, as well as increased ratio of immature neutrophils to the mature ones, or I/T ratio. Another factor that points to sepsis is a decreased absolute neutrophil count, or ANC. Additional diagnostic tests may include chest X-ray, blood glucose levels, and CRP.
The treatment of neonatal sepsis aims at addressing the underlying infection. This can be done by administering intravenous broad-spectrum antibiotics, which should then be switched to a more specific antibiotic once the causative organism is identified. It’s also important to support the newborn with fluids, supplemental oxygen, and in severe cases, mechanical ventilation.
Alright, so let’s talk about the nursing care you’ll be providing for a newborn with neonatal sepsis. Your priority nursing goals are to assist in eliminating the causative organism, provide supportive care, monitor for complications, and provide emotional support.
Now, in order to provide treatments to eliminate the causative organism, you will need to first collect blood, urine, and cerebrospinal fluid specimens, as ordered, and send them to the lab for analysis and culture. Then, administer the prescribed IV fluids and antibiotics.
Also, institute measures to provide supportive care during treatment. Promote temperature stability by placing the infant in an incubator or radiant warmer with an abdominal skin temperature monitor, and check their temperature frequently.