Nephrotic syndrome: Nursing
Nephrotic syndrome: Nursing
Acute Final
Acute Final
Notes
| NEPHROTIC SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
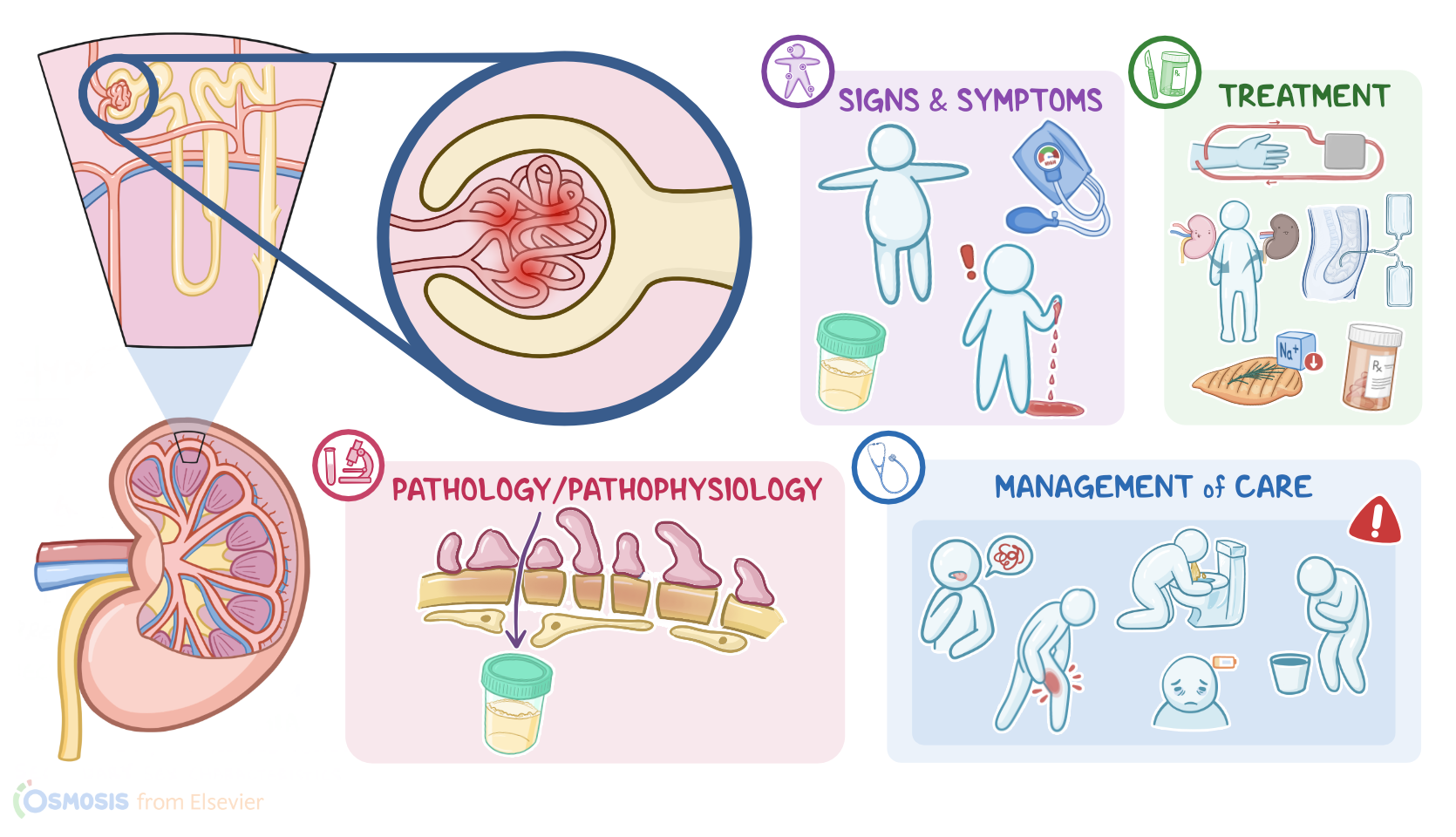
Nephrotic syndrome is a disorder characterized by a constellation of signs and symptoms caused by conditions that affect the tiny glomeruli in the kidneys, resulting in excessive loss of protein through urine, called proteinuria.
First, let’s quickly review some kidney physiology! Remember that the nephron is the functional unit of the kidney, and its role is to filter waste products and water from the blood. Each nephron is made up of a renal corpuscle and a set of renal tubules, which are, in order: the proximal convoluted tubule, the loop of Henle, the distal convoluted tubule and finally, the collecting ducts which drain urine into the renal papillae and eventually empty into the renal pelvis. The renal corpuscle is made up of the glomerulus, which is a bundle of capillary loops, and Bowman’s capsule, which surrounds the glomerulus. Now, blood enters the glomerulus through the afferent arteriole, then inside the glomerulus, glomerular filtration occurs. Then, the remaining blood exits the glomerulus through the efferent arteriole. The glomerular capillary wall is a semi-permeable membrane with three layers: the endothelium, which is the inner layer; the basement membrane; and the epithelium, which is the outermost layer. For filtration to occur, the endothelial and epithelial cells that line the capillary wall are separated by small pores that filter water and small particles from the blood and into the Bowman capsule. Only small particles are filtered from the blood and never proteins, since they are larger molecules. Also, normally, there aren’t any red blood cells in the urine. For glomerular filtration to occur, the hydrostatic pressure created by the blood pressure needs to be greater than opposing forces, such as the tubular filtrate and oncotic pressure, which is the pressure of proteins. The final product of filtration is called filtrate or primary urine, which will flow through the Bowman capsule into the proximal convoluted tubule.
Ok, now, some of the most common causes of nephrotic syndrome includea cute glomerulonephritis, focal segmental glomerulosclerosis, and minimal change disease, as well as diabetes and systemic lupus erythematosus.
Other causes include some cancers such as Hodgkin lymphoma; certain infections like those caused by Streptococcus species or HIV; as well as some drugs, such as NSAIDs and penicillamine. Lastly, nephrotic syndrome that occurs during the first year of life has a genetic basis.
And now, let’s look at the pathology of nephrotic syndrome. Regardless of cause, the hallmark feature of nephrotic syndrome is damage to the glomerular basement membrane, which increases its permeability. This allows proteins to make their way past the membrane and into the urine. Proteinuria, hypoalbuminemia, edema, hypertension, and hyperlipidemia develop as a consequence.
As total serum protein levels, specifically the protein albumin, decrease, there’s a lower oncotic pressure in blood vessels, which causes edema that can eventually progress to generalized swelling in the entire body, called anasarca. Additionally, the diminished oncotic pressure stimulates lipoprotein synthesis in the liver, causing hyperlipidemia.
Other proteins, like antibodies, are also lost in the urine This means the immune response is also altered in nephrotic syndrome, so the client is at risk for infections.Additionally, important anticoagulant proteins are lost through urine, so another result of nephrotic syndrome is a state of hypercoagulability, which can increase the risk for arterial and venous thromboembolism, like deep vein thrombosis, renal vein thrombosis or even pulmonary embolism. Paradoxically, there’s also an increased risk of bleeding with nephrotic syndrome, because proteins such as coagulation factors are also lost through the urine. Finally, calcium also tends to be lost through urine, causing hypocalcemia.
Now let’s translate that into a clinical picture. Edema initially manifests as periorbital or facial edema. Fluid retention can become generalized or build up in the abdominal cavity, which causes ascites. And all that gradual accumulation of fluid in the body causes weight gain.
Additionally, because of hyperlipidemia, fat bodies or fatty casts often appear in the urine, causing foamy urine, and urine output may decrease. Finally, clients can develop hypertension, though blood pressure may be decreased if the client is hypovolemic, and they may bleed for longer than normal following an injury.
The diagnosis of nephrotic syndrome starts with the client’s history and physical assessment. A 24 hour urine collection shows severe proteinuria, with more than 3.5 g/dL of protein in a 24 hour urine sample. Clients also have serum albumin levels below 3 g/dL as well as hyperlipidemia. There are also abnormalities in the coagulation panel, such as an increased PT, aPTT, and INR. Creatinine and blood urea nitrogen are also usually increased, and GFR is decreased. Last but not least, a kidney biopsy can be done to establish the cause of nephrotic syndrome.
Treatment of nephrotic syndrome depends on the cause. General treatment includes nutrition therapy, immunosuppressants, and symptomatic treatment. Nutrition therapy includes a low sodium diet, moderate protein intake and fluid restriction in the case of significant edema. Corticosteroids such as prednisone, as well as other immunosuppressants like cyclophosphamide can be used to help induce remission.