Newborn adaptation to extrauterine life: Nursing
Notes
| NEWBORN ADAPTATION TO EXTRAUTERINE LIFE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| FETAL CIRCULATION |
| |
| RESPIRATORY ADAPTATION |
| |
| CARDIOVASCULAR ADAPTATION |
| |
| APGAR SCORE |
| |
Transcript
During intrauterine life, the placenta supplies the fetus with oxygen and nutrients essential for its growth and development. After birth, this supply ceases, the infant has to adapt to the extrauterine environment. The main changes during this adaptation period include those of the respiratory and cardiovascular system.
Now, in order to understand the changes that take place during transition to extrauterine life, let’s review some key differences between fetal and newborn circulation. Remember that during intrauterine life, the fetal lungs are not functional in terms of gas exchange. Instead, they are filled with fluid, and the arteries in the lung are constricted, resulting in high vascular resistance in the lungs. Because of this high pressure, relatively little blood reaches the lungs. Because no gas exchange occurs in the lungs, the fetus needs to get oxygen from the placenta.
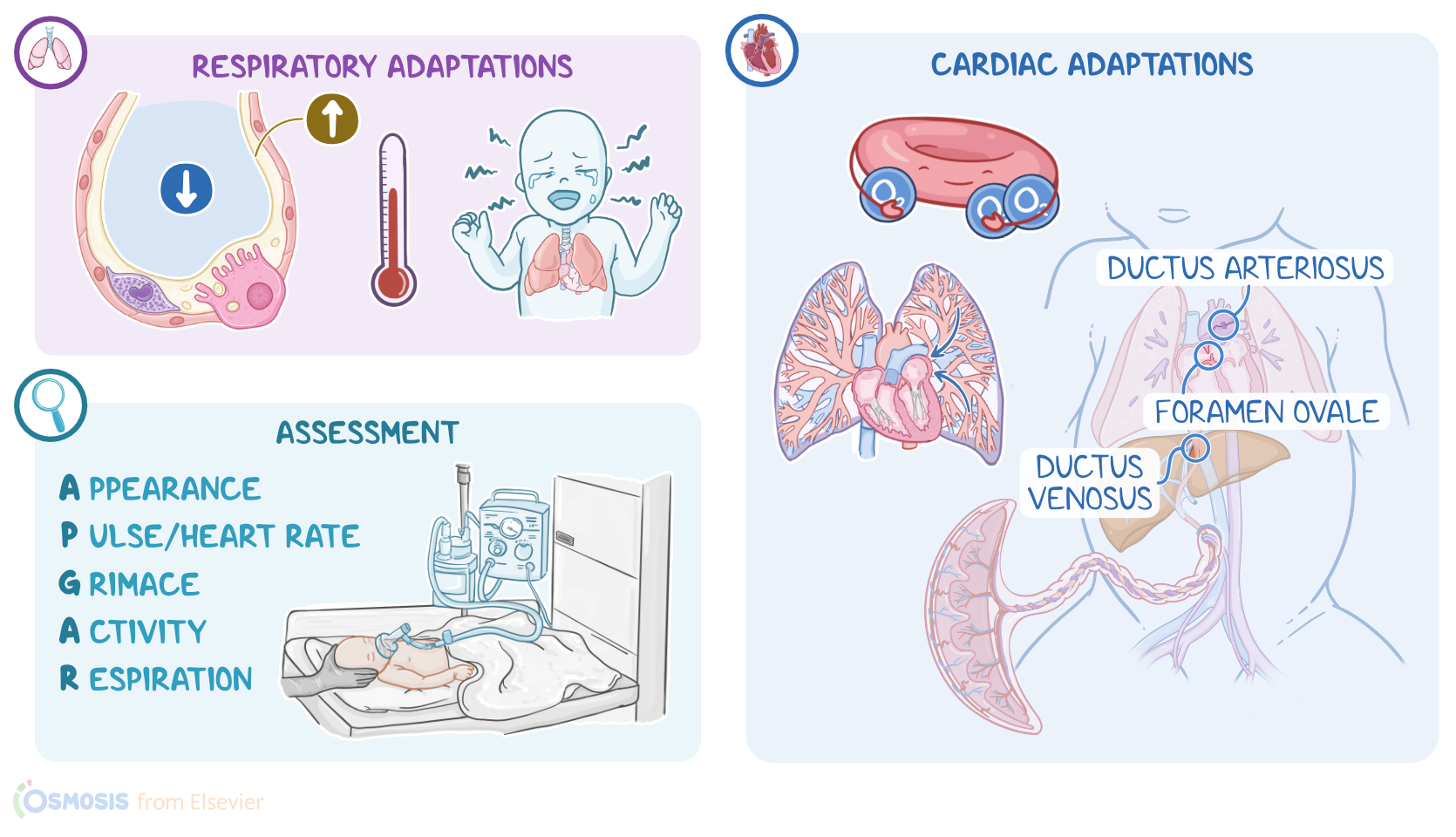
Now, there are three fetal shunts to help divert most of the blood away from the lungs, while maximizing the delivery of oxygenated blood to key organs like the brain and heart. First is the ductus venosus that connects the umbilical vein to the inferior vena cava, thus allowing most of the oxygenated blood to bypass the liver and travel up to the heart. Next is the foramen ovale in the atrial septum, that allows blood from the right atrium to flow directly into the left atrium. This allows oxygenated blood to bypass the non-functional lungs and get pumped to the rest of the body instead by the left ventricle. The last shunt is the ductus arteriosus which connects the pulmonary artery to the aorta and also helps bypass the lungs.
The liver and lungs still receive enough blood to keep their tissue healthy and growing, but the three shunts allow large quantities of blood to bypass them and help the fetus optimize its limited oxygen and nutrient supply.
Now, toward the end of gestation, the fetal lungs start to prepare for extrauterine life. First, there’s increased production of surfactant, a mixture of lipids and proteins that help prevent collapse of the alveoli, is increased. The lungs also decrease the production of fetal lung fluid, a liquid that fills the fetal lungs during gestation that enables normal fetal lung development; and the lungs start the process of removing the fluid out of the alveoli and into the interstitial space. Together these actions help prepare the lungs to receive oxygen when the baby takes its first breath.
Now, during the birth process, there are several types of stimuli that help support the newborn’s respiratory adaptation. First is thermal stimulation. During gestation, the fetus lives in a warm, intrauterine environment; but after birth, the infant emerges into a much colder extrauterine environment. This abrupt change in the temperature is detected by thermoreceptors in the infant’s skin and subsequently stimulates the respiratory center in the medulla. There are also other kinds of sensory stimulation after birth, such as exposure to light and sound, as well as tactile stimulation from labor contractions as the fetus descends through the birth canal, and as the newborn is quickly dried off immediately after birth. All of these help trigger the infant’s first breath. The increased intrapulmonary pressure produced by the infant’s first breaths help force any remaining fluid out of the lungs.
Okay, let’s switch gears and move on to cardiac adaptation. With the cutting of the umbilical cord at birth and the onset of respirations, the oxygen content in the blood increases dramatically. Oxygen is a potent pulmonary vasodilator, and as the pulmonary vessels dilate, pulmonary vascular resistance decreases. This allows increased blood flow through the lungs, increased venous blood flow to the left atrium, and higher left atrial pressure. Increased left atrial pressure promotes the closure of the foramen ovale. Oxygen is also a potent constrictor of the ductus arteriosus so with the baby’s first breath, it slowly begins to close, thus preventing blood shunting from the pulmonary artery into the aorta.
Now, the cutting of the umbilical cord also causes the umbilical vein and the ductus venosus to collapse because of absent blood flow. There is also an increase in systemic vascular resistance and increased systemic oxygen content, causing the umbilical arteries to vasoconstrict. Eventually all fetal shunts and the umbilical arteries and vein undergo fibrotic changes and close completely.