Omphalocele and gastroschisis: Nursing
Introduction0:00–0:27
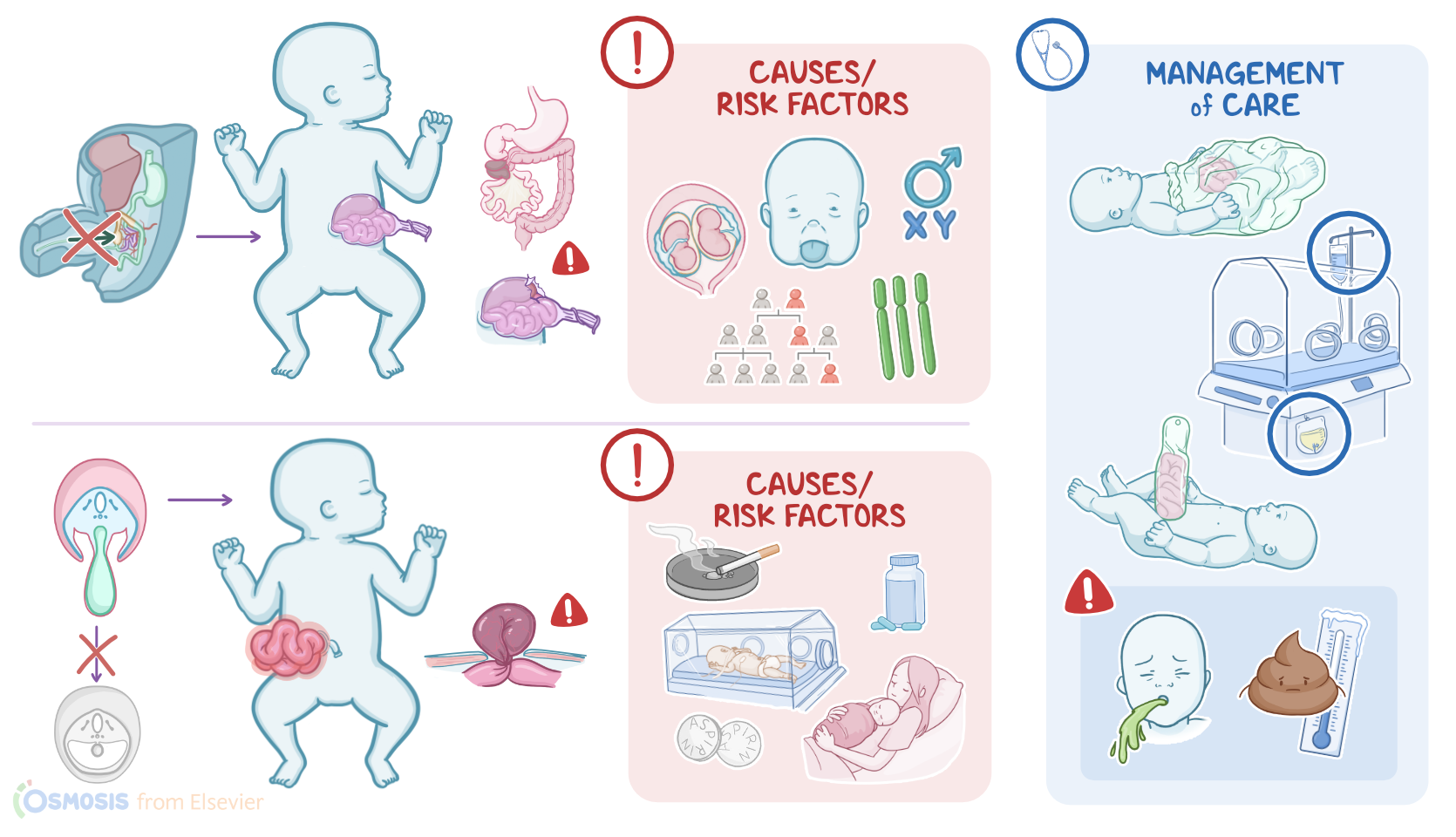
Omphalocele and gastroschisis are both congenital abdominal wall defects. An omphalocele is an umbilical ring defect where the abdominal contents, such as the gastrointestinal tract or liver, can protrude into an external peritoneal sac.
Alternatively, in gastroschisis, the abdominal contents slip outside the abdomen without a sac.Alright, let’s quickly review the physiology of the development of the abdominal wall.
Physiology0:27–1:36
From the outside in, the abdominal wall is formed by the skin, superficial fascia, muscles, the deep fascia, and the parietal peritoneum which lines the abdominal cavity.
During the third to fourth week of fetal development, the embryo starts to change shape from a flat, three-layer disc to something more shaped like a cylinder, a process called embryonic folding.
In the horizontal plane, the two lateral folds eventually come together and close off at the midline, except for at the umbilicus, where the umbilical cord connects the fetus to the placenta.
This folding allows for the formation of the gut within the abdominal cavity. During around the sixth week of development, the liver and intestines grow really quickly, and because the abdominal cavity is still pretty small, there’s limited space, which causes the midgut to herniate through the umbilical ring into the umbilical cord, and this happens normally.
At about week 10, though, the abdominal cavity typically has grown enough to allow the midgut to come back from the umbilical cord.Now, the causes of omphalocele and gastroschisis are mostly unknown, but they are associated with certain conditions or environmental exposures.
Causes & risk factors1:36–2:35
Omphaloceles are associated with genetic and chromosomal abnormalities such as Trisomy 13, 18, or 21, or Beckwith-Wiedemann syndrome which is a genetic condition where the infant grows larger than normal.
Meanwhile, gastroschisis is rarely associated with genetic conditions but instead is related to fetal exposure to nitrosamines in tobacco and cyclooxygenase inhibitors like aspirin and ibuprofen.
Risk factors for omphalocele include maternal age less than 20 or more than 40, multiple gestation, family history, and clients assigned male at birth.
In contrast, the risk of gastroschisis is increased for young mothers with their first child. Finally, additional risk factors for gastroschisis include prematurity.Moving on to pathology, omphalocele develops when the abdominal wall fails to close properly during development and then this large abdominal wall defect results in the midgut failing to rotate and return into the cavity.
Pathology2:35–4:15
Other contents, like the liver, might then also herniate into the umbilical cord. Over time, this can lead to several complications including injury to herniated organs such as liver injury, intestinal atresia or stenosis, bowel perforation, and necrosis.
Another complication of omphalocele is malrotation with volvulus, which occurs when the midgut doesn’t rotate in the way it should and twists around itself, leading to intestinal obstruction, infarction, and necrosis.
The abdominal cavity may also become malformed or the sac around the herniated organs may rupture. A large omphalocele can even affect the respiratory system, such as inducing pulmonary hypoplasia where lungs do not grow to full capacity.In contrast, gastroschisis occurs when the abdominal wall fails to form normally during the embryonic period, leaving a hole typically to the right of the umbilicus.
This makes it easy for the abdominal contents, like the intestines, stomach, and liver, to protrude through the abdominal wall.
In contrast to omphaloceles, these are not covered by a peritoneal layer and are exposed to amniotic fluid. As a result, the intestines may get irritated and inflamed, which can lead to malabsorption issues.
Finally, sometimes, when the bowels herniate, it can compromise their blood supply, which can lead to infarction of the intestinal wall.Now, the clinical manifestations for both omphalocele and gastroschisis include a mass protruding from the abdomen.
Clinical manifestations4:15–5:02
In omphalocele, the abdominal mass is typically in the anterior midline at the site of the umbilical cord. It is often covered by a membrane of amnion and peritoneum and can contain intestinal loops or parts of other abdominal organs like the liver.
In contrast, gastroschisis is a full-thickness para-umbilical abdominal wall defect, typically to the right of the umbilicus.
The bowel that is protruding out often is thick, matted, and doesn’t have any membrane covering it. In addition, some infants may experience difficulty feeding or passing stool, as well as respiratory distress if pulmonary hypoplasia is present.The diagnosis of omphalocele and gastroschisis starts with the client’s history and physical assessment.
Diagnosis5:02–5:26
When still in utero, additional tests involved include both imaging, such as intrauterine ultrasonography or MRI, and fluid testing, including amniocentesis and a blood test for maternal serum alpha-fetoprotein or MSAFP which is typically increased.
Treatment of omphalocele and gastroschisis focuses on correcting the defect and providing supportive care. The client is typically given IV fluids and nutrients, as well as antibiotics to prevent or treat infections.
Treatment5:26–5:55
Typically, the intestines are placed into a silastic silo which positions them above the opening in the abdominal cavity so gravity can help move the contents back into the cavity.
Finally, surgery is often required to place the remaining organs into the abdominal cavity.Alright, let’s talk about the goals of care for a client with omphalocele or gastroschisis.
Management and care5:55–7:33
Your initial goals of care are to minimize heat and fluid loss; prevent complications; promote client comfort. Immediately after birth, minimize heat and fluid loss from the exposed bowel by placing the newborn feet first into a sterile bowel bag and securing the bag at nipple level.
Then, place them in an isolette with temperature control, and monitor their temperature frequently. Infuse the prescribed IV fluids to replace insensible fluid losses, and place an indwelling urinary catheter to monitor fluid output.Also be sure to prevent complications by administering the prescribed antibiotics to prevent infection.
To prevent bowel distention, maintain NPO status; place a nasogastric tube to low continuous suction; and administer the prescribed parenteral nutrition.
Also be sure to position the infant on their side during initial care to avoid occluding the mesenteric blood flow and bowel ischemia.
Notify the healthcare provider immediately for a dusky, dry, or cool bowel. Finally, be sure to promote comfort while providing care.
Decrease environmental stimuli by reducing light and noise and by clustering activities to allow periods of rest. Assess the infant frequently for signs of pain using an appropriate pain scale, like the Neonatal Pain, Agitation, and Sedation Scale or N-PASS; and administer the prescribed analgesics.Okay, moving on to the teaching you’ll provide for the caregivers.
General client and family teaching7:33–8:16
Begin by explaining that gastroschisis and omphalocele are defects where part of the baby’s internal organs come through an abnormal opening in the abdomen.
Be sure to provide clear explanations about how the organs will slowly move back into the abdomen, and then the opening will be closed surgically.
When their baby is ready to go home, be sure to teach them about care for their baby at home, including medications and feedings.
Instruct them to seek medical attention right away if their baby isn’t eating well, doesn’t gain weight or has trouble having bowel movements.
Also teach them to seek emergency care if there are signs of a bowel obstruction, including green, or bilious vomit. Alright, as a quick recap...
Omphalocele and gastroschisis are congenital abdominal wall defects characterized by abdominal contents protruding outside the body.
Review8:16–9:27
With omphalocele, an umbilical ring defect allows the viscera to protrude into an external peritoneal sac. In gastroschisis, abdominal contents protrude outside the body without a sac.
Causes of these conditions aren’t known, but risk factors include advanced or very young maternal age, multiple gestation, family history, and being assigned male at birth, as well as fetal exposure to nitrosamines in tobacco and cyclooxygenase inhibitors like aspirin and ibuprofen.
Diagnosis involves a history and physical, in utero-testing including ultrasound, MRI, amniocentesis, blood levels of maternal serum alpha-fetoprotein, as well as after-birth imaging like X-ray or CT scan.
Treatment focuses on correcting the defect along with supportive care. Goals of nursing care include minimizing heat and fluid loss; preventing complications; and promoting client comfort.
Teaching centers on learning about the defect,
| OMPHALOCELE AND GASTROSCHISIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below