Osteoarthritis: Nursing
Osteoarthritis: Nursing
Watch later
Watch later
Notes
| OSTEOARTHRITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Osteoarthritis, also known as degenerative joint disease, is a chronic, non-inflammatory condition characterized by gradual wear and tear of joint cartilage and underlying bone followed by inadequate repair. In fact, it is the most common type of arthritis overall.
Now, let’s go over some anatomy and physiology. Joints can be classified into three main groups based on their structure and range of movement. Fibrous or synarthrodial joints, like the joints between the bones of the skull, generally don’t move at all. On the other hand, cartilaginous or amphiarthrodial joints, like the joints of the spine, allow for some movement. Finally, synovial or diarthrodial joints, like those of the wrist, elbow, shoulders, hips, knees, and ankles, are freely movable.
Now, zooming in, the bones of healthy synovial joints are connected via a fibrous capsule that is continuous with the periosteum, which is the outer layer of bones. The fibrous capsule has an inner lining called the synovial membrane; this membrane consists of connective tissue and specialized cells that remove debris and produce synovial fluid, which is a viscous fluid found inside the joint capsule to lubricate the joint. In addition, the bones are covered with a layer of articular cartilage, which is a type of connective tissue with a lubricated surface that acts like a protective cushion for bones to smoothly glide against.
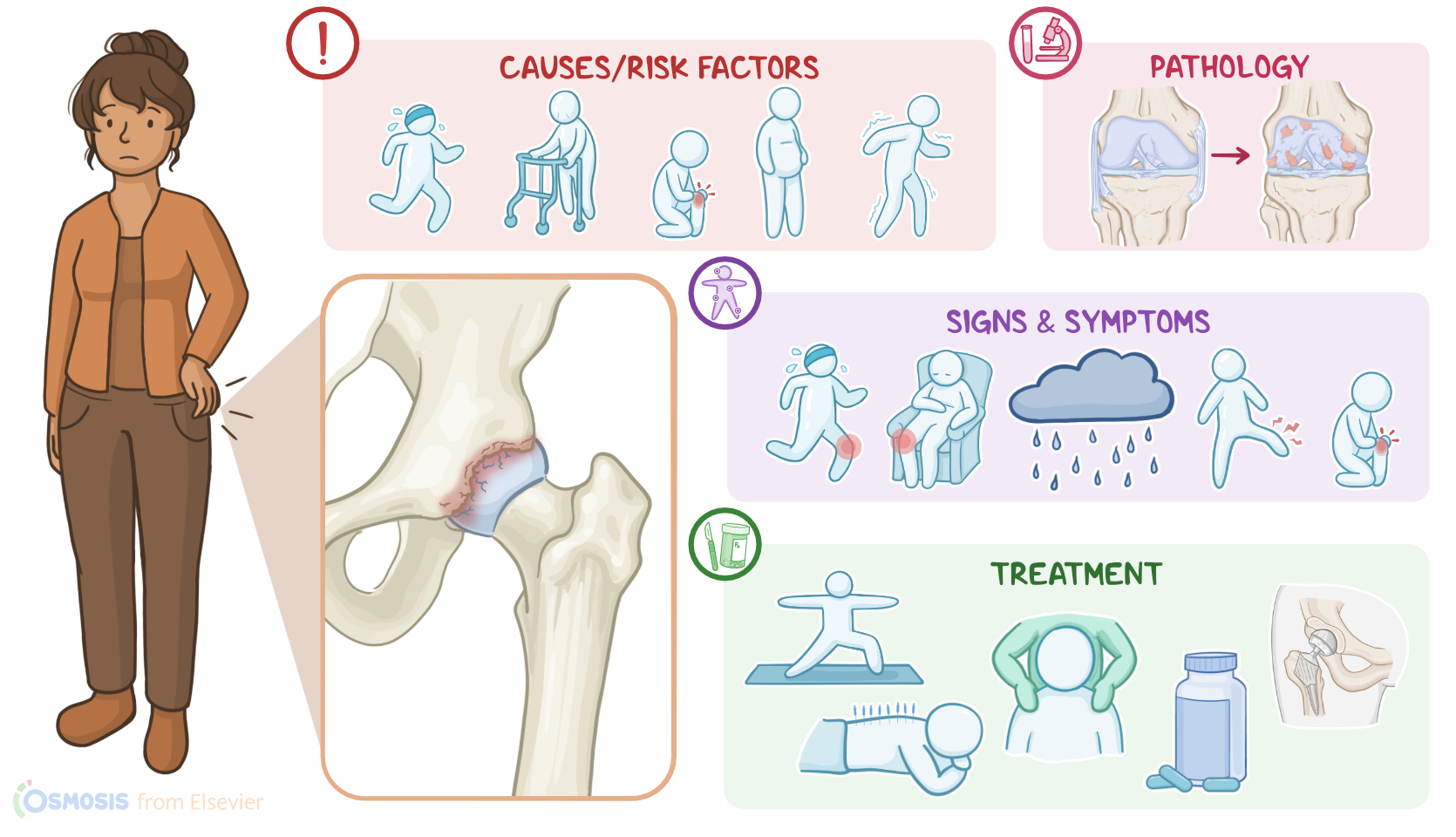
Now, the main cause for osteoarthritis seems to be the daily stress applied to synovial joints throughout an individual’s lifetime, especially to weight-bearing joints like those of the hip, knee, and ankle. This is why the biggest risk factor for osteoarthritis is age, especially after 50 years; alongside obesity, joint overuse or injury, and altered walking patterns, which can increase joint stress.
Other risk factors include a family history of osteoarthritis; being assigned female at birth; and having associated medical conditions, such as metabolic disorders like diabetes, neurologic disorders like multiple sclerosis, or hematologic disorders like sickle cell disease.
Now, the pathology of osteoarthritis occurs when the articular cartilage wears away from repetitive stress, becoming weaker and losing elasticity. Since cartilage has limited repair capacity, the areas of maximal stress start developing fibrillations, which are cracks or clefts on what used to be a smooth articular surface. So, over time, the cartilage will continue to erode away until the underlying bones are exposed, allowing them to rub against each other. At the same time, on the joint edges, bone reacts by growing outward at the margins, forming what’s called osteophytes or bony spurs.
The main symptom of osteoarthritis is joint pain. In the early stages of the disease, this pain tends to worsen with activity and is much more pronounced in the evening; and over time, clients may also experience pain with slight motion or even at rest. Sometimes, joint pain can get worse with weather changes. Another classic symptom is joint stiffness with limited range of motion, which is often more pronounced in the morning, and typically lasts up to 30 minutes; stiffness also improves with activity as the joint warms up. Additional symptoms include joint swelling or instability, which might make it harder for the client to perform their daily activities.
Finally, osteophytes might be visible as single subcutaneous nodules over the affected joints. Osteophytes in the distal interphalangeal joints are called Heberden nodes; while in the proximal interphalangeal joints, they are called Bouchard nodes.
Diagnosis of osteoarthritis starts with the client’s history and physical assessment, followed by X-rays of the affected joints to confirm the diagnosis by showing cartilage loss and narrowing of the joint space. Additional diagnostic studies include blood tests, which are typically normal, but are required to rule out other types of arthritis and to reveal any associated medical conditions causing osteoarthritis. In some cases, arthrocentesis might be done to evaluate the synovial fluid and rule out other types of arthritis; in osteoarthritis, the synovial fluid is usually clear and has no signs of inflammation.
Although the joint damage in osteoarthritis can’t be reversed, certain treatment options can be used to stop its progression, as well as to help mitigate some of the symptoms, and improve the client’s quality of life. These treatment options can involve lifestyle modifications, like weight-loss, moderate exercise, as well as physical therapy, involving range of motion exercises and local muscle strengthening. This can be especially important when large weight-bearing joints like the hips and knees are affected.
For clients experiencing joint instability, the joint can be immobilized and protected using supportive or orthotic devices, such as braces and splints. Alternative treatments might also include acupuncture, meditation, yoga, massage, and heat application. Next, pharmacological treatment is mainly symptomatic, focusing on reducing pain by using oral analgesics like NSAIDs and acetaminophen, topical capsaicin, or weak opioids like tramadol. Some clients might also benefit from injections of corticosteroids into the joint.