Pain management during labor: Nursing
Notes
| PAIN MANAGEMENT DURING LABOR | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
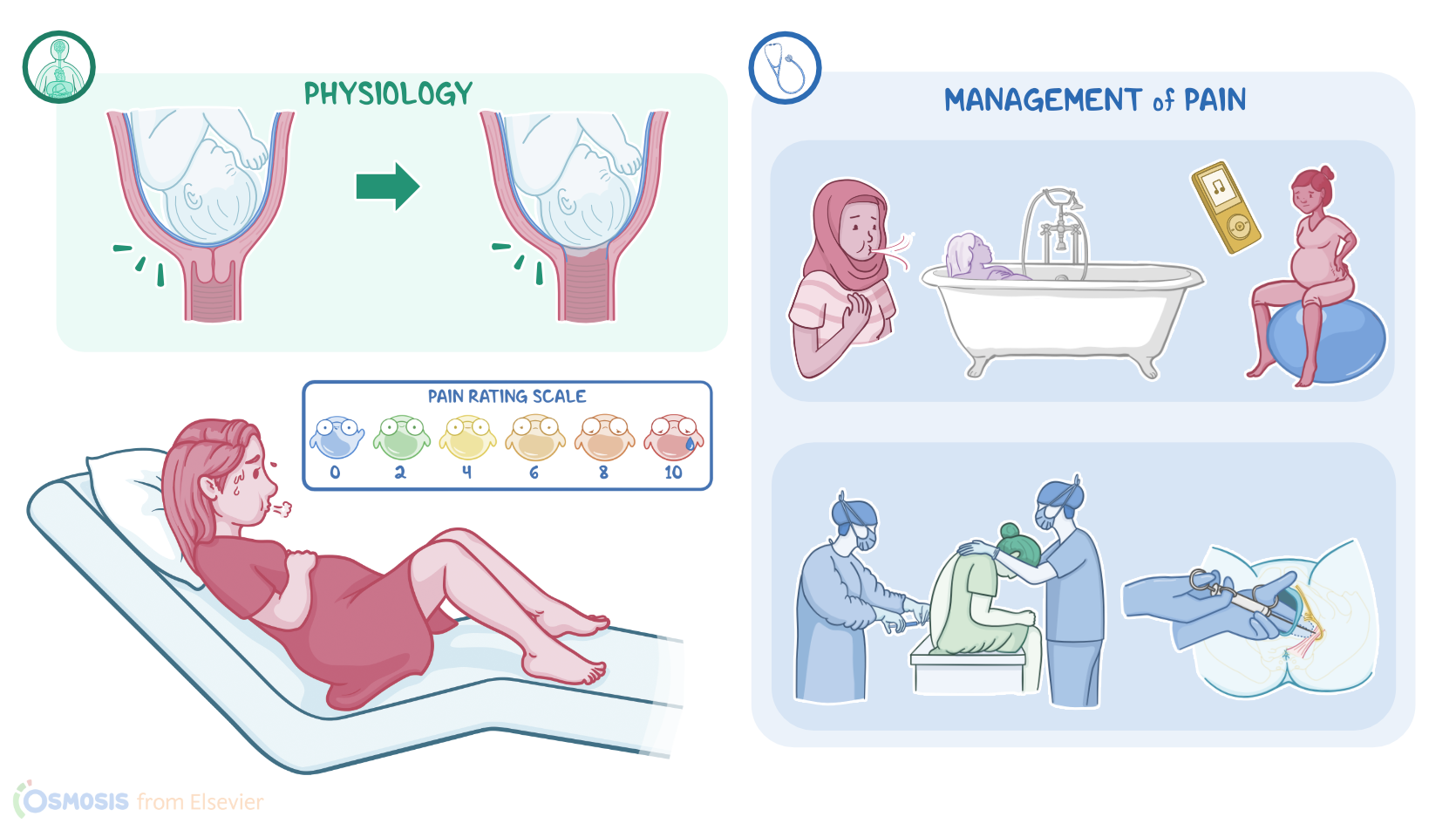
| PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Labor refers to a series of progressive contractions of the uterus that result in dilation and thinning of the cervix. This, in turn, allows the fetus to descend from the uterus, through the birth canal, and into the extrauterine environment. This process results in pain that can be managed in a variety of ways. Now, from a physiological standpoint, not only is labor pain normal, but it’s also easily anticipated, allowing time for preparation and acquisition of skills to help manage it. Secondly, although intense, labor pain is also time limited. It is usually intermittent and decreases rapidly after hitting its peak. Finally, it will end with the birth of a child, which is highly motivating for the mother, allowing for a higher pain threshold.
Pain during labor can be either visceral or somatic. Visceral pain mostly occurs during the first stage of labor due to uterine contractions that lead to hypoxia of the uterine muscles, dilation of the cervix, distension of the lower uterine segment, as well as pressure and pulling on pelvic structures such as the fallopian tubes, ovaries, and bladder. Then, somatic pain mostly occurs during the later part of the first stage and second stage of labor, as the uterine contractions become more intense. Also during this time, pain is increased as the fetus pushes directly on maternal tissues like the vagina, perineum, and the lumbosacral plexus during its descent.
Now, pain during labor can cause anxiety leading to a stress response that can have an adverse effect on the progression of labor and on the fetus. Excessive pain can heighten the individual’s fear and anxiety, causing the release of cortisol and catecholamines like epinephrine and norepinephrine. When these act on alpha receptors, the uterine blood vessels and muscles constrict, reducing uterine blood flow, reducing the fetal oxygen supply, and potentially leading to fetal hypoxia. Labor also increases the mother’s metabolic rate and demand for oxygen, making the hypoxia worse. Finally, after labor, poorly managed pain can make it difficult to interact with the newborn due to post-labor fatigue and exhaustion.
Now, management of labor pain begins with prenatal education, by offering realistic information on pain and expectations, as well as analgesia and anesthesia techniques. This can reduce anxiety and allow partners to rehearse for labor and develop the necessary skills to cope with labor pain. Options for pain management can be pharmacological or non-pharmacological. Non-pharmacological measures include cognitive processes and cutaneous techniques. Cognitive processes include continuous labor support, where the presence of a support person provides emotional and physical support during labor; and music therapy, which can increase pain tolerance and serve as a distraction from pain.
Other cognitive processes include relaxation techniques that can be used to conserve energy and decrease fatigue. These include guided imagery, where the client focuses on a pleasant mental scene or experience; as well as breathing techniques that can be done either during or between contractions, such as taking a deep breath through the nose then gently exhaling through pursed lips. On the other hand, cutaneous techniques can be used to modulate the intensity of pain by helping to block pain impulses and stimulating the release of endorphins. These include back, shoulder, or sacral massage; the use of a birthing ball, which can be used to rock or gently bounce on to decrease perineal pain; and hydrotherapy which uses warmth and buoyancy to promote relaxation and increase pain tolerance.
Moving on, there are four types of pharmacologic methods to keep in mind. First, there are systemic analgesics, which can include IV administration of full opioid agonists like fentanyl and remifentanil; or partial opioid agonists like butorphanol and nalbuphine. Next, there’s neuraxial or regional analgesia, which involves either an epidural or spinal administration of a local anesthetic and an opioid medication; sometimes it can be a combination of epidural and spinal administration. Another type of regional analgesia is a pudendal block, which involves injecting a local anesthetic just below the ischial spine through the vaginal wall. Next, there’s intermittent inhalation of nitrous oxide which provides pain relief but the client remains conscious. The final method is general anesthesia where the patient is fully unconscious so the most common scenario for its use is for cesarean delivery.