Ovarian cancer: Nursing
Ovarian cancer: Nursing
Medical Surgical
Medical Surgical
Notes
| OVARIAN CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| CAUSES AND RISK FACTORS |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
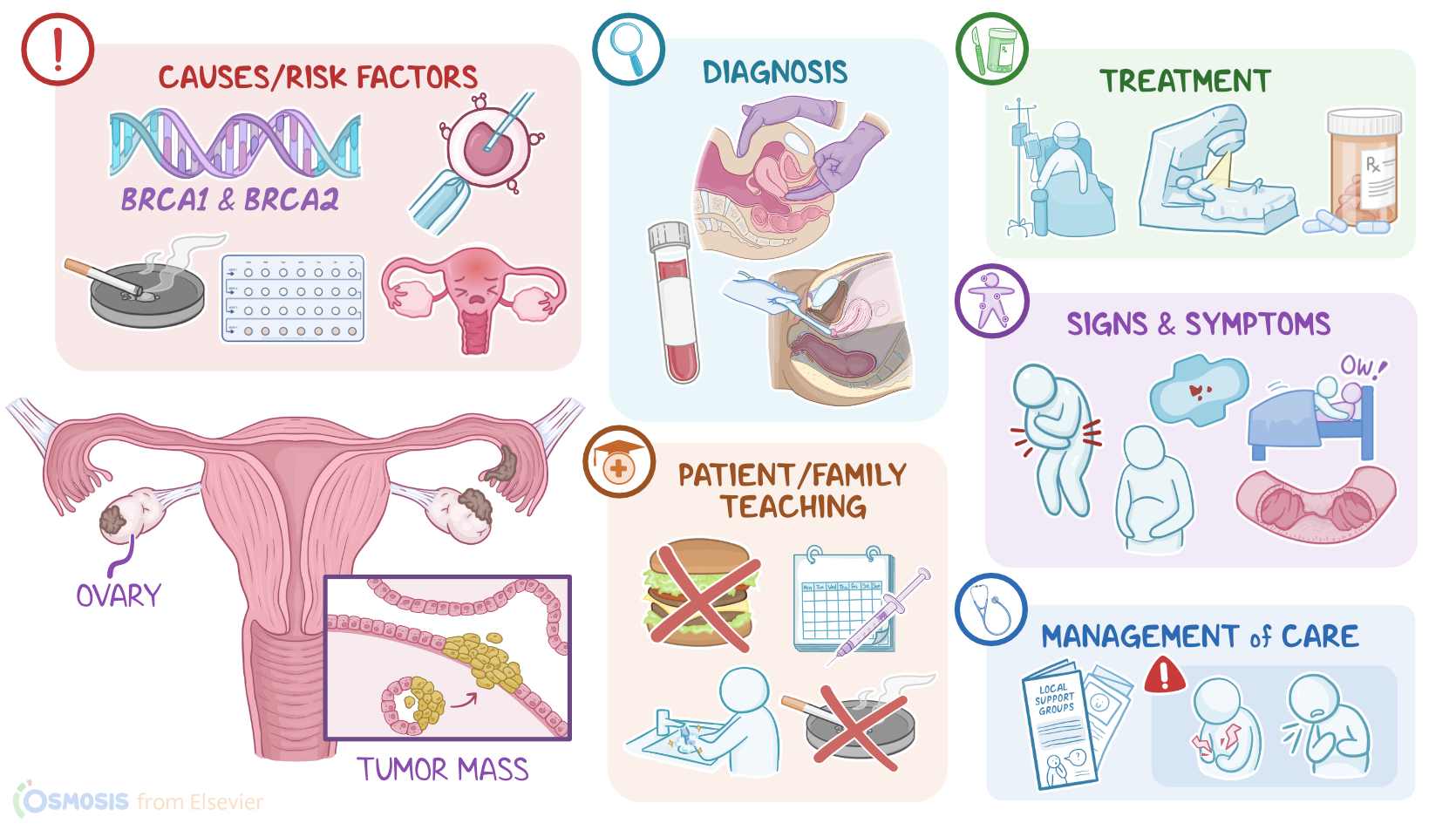
Ovarian cancer is a malignant cell growth that begins in the ovaries or the fallopian tube. It is often bilateral and spreads quickly to nearby organs through direct extension, to abdominal organs through abdominal seeding, and to distant organs through the blood and lymphatic vasculature.
Now, let’s recap the anatomy and physiology of the ovaries, which are paired almond-shaped organs that lie within the pelvic cavity, on each side of the uterus. The functions of the ovaries include producing and releasing oocytes through the process of oogenesis, in addition to producing estrogen and progesterone, which are responsible for maintaining pregnancy, growth, and development in assigned females at birth.
Now, let’s look at the microscopic structure of the ovaries. Each ovary is lined by a simple squamous epithelium called the germinal epithelium, which is then covered by a thick connective tissue capsule called the tunica albuginea. The inside of the ovary is divided into two zones: cortex and medulla. The cortex houses small sacs of oocytes and supporting cells called the ovarian follicles, which are embedded in the outer layer of a unique type of connective tissue called the ovarian stroma.
Now, the exact cause of ovarian cancer is unknown, but there’s typically a genetic mutation in a cell of the ovary or the fallopian tube, such as a mutation in breast cancer genes 1 and 2, also known as BRCA1 and BRCA2 genes.
These mutations may arise from a variety of risk factors. Nonmodifiable risk factors include middle or older age, family history, early menarche, late menopause, a history of polycystic ovarian syndrome or PCOS, endometriosis, breast, or colon cancer.
On the other hand, modifiable risk factors include smoking, obesity, hormone replacement therapy, and ovarian hyperstimulation from infertility treatments like in vitro fertilization, as well as pelvic inflammatory disease, nulliparity, and first pregnancy at an older age.
Now, all these risk factors can lead to dedifferentiation of the surface ovarian epithelium or the fallopian tube epithelium.
This can be explained by the incessant ovulation theory, which suggests that the risk of ovarian cancer increases with each cycle of ovulation. During ovulation, the follicle ruptures and releases the mature oocyte, which inadvertently causes damage to the surface epithelium.
This damage can lead to the formation of cortical inclusion cysts, which are invaginations of the ovarian surface epithelium. And the epithelial cells of these cysts may then start dividing uncontrollably, forming a tumor mass.
As the tumor keeps growing, it can start invading neighboring tissues, and may even spread to nearby lymph nodes, or metastasize to distant organs such as the brain. Ovarian cancer can also spread to abdominal organs through abdominal seeding and thoracic organs through transdiaphragmatic passage.
Initially, clients with ovarian cancer can be completely asymptomatic or experience subtle and non-specific symptoms. Common early symptoms can include abdominal distension, bloating, abdominal or pelvic pain, in addition to urinary frequency and urgency.
Later on, ovarian tumors can cause unintentional weight loss, abdominal enlargement, bowel obstruction, menstrual changes, and dyspareunia, which is pain during sexual intercourse. A classic finding is a “sister mary joseph nodule”, which happens when it metastasizes to the umbilicus.
The diagnosis of ovarian cancer starts with the client’s history and physical assessment, including bimanual pelvic examination, which may show signs of enlarged ovaries, followed by additional diagnostic tests like transvaginal ultrasound to observe the tumor. Laboratory test results are generally non-specific and may show elevated blood levels of tumor markers like CA125, inhibin, alpha-fetoprotein, or AFP, and beta-human chorionic gonadotropin, or hCG for short. Additional imaging tests including CT scan, MRI, and positron emission tomography or PET can be used to stage the disease with the TNM classification, by defining the Tumor location and looking for lymph Node involvement or Metastasis. Ovarian cancer can also be staged using the FIGO system into stage 0, or carcinoma in situ; stage I, which is confined to the organ of origin; stage II, where the tumor has extended to adjacent organs or tissues; stage III, where the tumor has spread to lymph nodes or nearby tissues within the pelvis; and lastly, stage IV, characterized by distant metastasis beyond the pelvis. Finally, exploratory laparotomy with biopsy can be done in order to confirm the diagnosis. Now, the definitive treatment of ovarian cancer is total abdominal hysterectomy with bilateral salpingo-oophorectomy; this is a type of surgical procedure that involves the complete removal of the uterus, in addition to both fallopian tubes and ovaries. In cases of lymph node involvement, they should also be removed. This surgical procedure is usually followed by chemotherapy and radiation therapy to kill any remaining cancer cells.
In addition, clients can also be given targeted therapy with medications called poly (ADP-ribose) polymerase or PARP inhibitors, which block the PARP enzyme that has a role in DNA repair; as a result, PARP inhibitors can prevent cancerous cells from repairing their DNA, ultimately causing these cells to die.
Alright, let’s look at the nursing care you’ll provide for a client with ovarian cancer. Your priority nursing goals are to provide postoperative care, administer the prescribed chemotherapeutic medications, and provide comfort and emotional support to promote quality of life.