Physiologic changes - Postpartum: Nursing
1,446views
Notes
| PHYSIOLOGIC CHANGES - POSTPARTUM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| WEIGHT LOSS |
| |
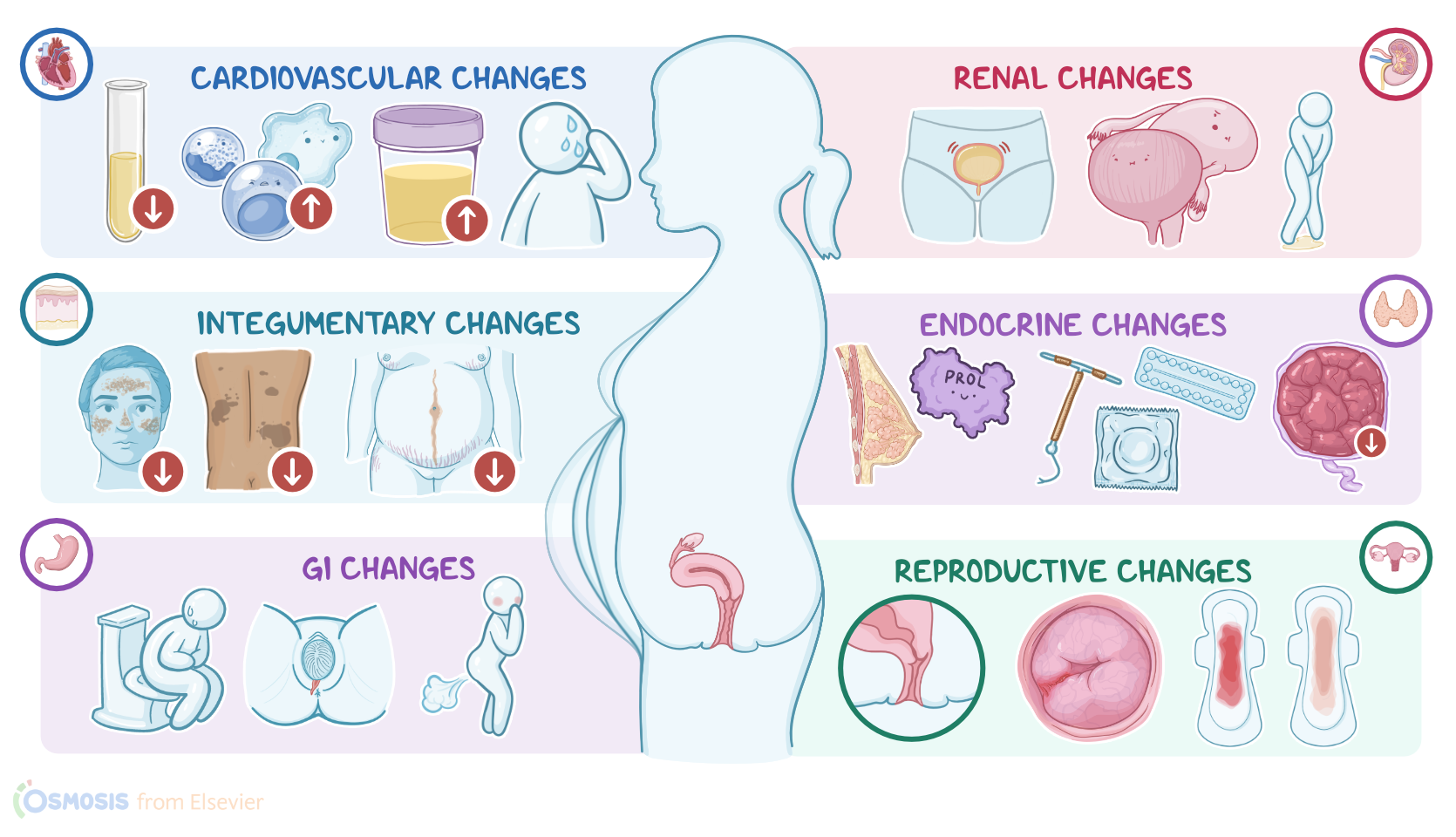
| REPRODUCTIVE CHANGES |
| |
| CARDIOVASCULAR & HEMOTOLOGICAL CHANGES |
| |
| GASTROINTESTINAL CHANGES |
| |
| RENAL CHANGES |
| |
| ENDROCRINE CHANGES |
| |
| INTEGUMENTARY CHANGES |
| |
| MUSCULOSKELETAL CHANGES |
| |
| NEUROLOGICAL CHANGES |
| |
Transcript
The postpartum period, also known as puerperium, is defined as the first six weeks after delivery. Physiologic changes during the postpartum period include the reversal of changes that occurred during pregnancy. Moreover, these changes are primarily caused by a rapid drop in estrogen and progesterone.
Now, after delivery, a client usually loses 4500 to 5800 grams or 10 to 13 lb, which covers the weight of the fetus, amniotic fluid, and the placenta. The weight loss starts immediately after delivery and continues over the next several months due to normalization of blood volume and increased caloric expenditure from milk production.
Okay, let’s focus on reproductive changes, starting with the uterus. After delivery, the uterus begins to return to its nonpregnant state of size and position, a process called uterine involution. As soon as the placenta is delivered, uterine muscle fibers constrict uterine blood vessels, preventing a life-threatening condition called postpartum hemorrhage. Uterine contractions, often referred to as afterpains because they cause sharp pain in the lower abdomen, continue during the postpartum period to further aid uterine involution. Now, clinicians can track the progress of involution by palpating the top part of the uterus, called the fundus. At about 12 hours after delivery, the fundus can be palpated at 1 cm above the umbilicus. After that, it normally descends by about 1 centimeter, or 1 fingerbreadth, per day, until it reaches the pelvic cavity by the 14th day.
Now, let’s take a look at vaginal discharge after birth, called lochia. There are three types; lochia rubra, lochia serosa, and lochia alba. Lochia rubra refers to the dark red vaginal discharge that is present for the first 3 days. It consists of blood, small blood clots, decidua, and mucus. As the bleeding reduces, the volume of vaginal discharge reduces, and lochia rubra transforms into lochia serosa.
Lochia serosa refers to the thin, red to brown vaginal discharge that lasts until the 10th day after delivery. It consists of white blood cells, serous exudate, and cervical mucus. As time passes, lochia serosa transforms into lochia alba.
Lochia alba refers to the yellowish-white vaginal discharge that typically lasts until the 14th day after delivery, but can persist up to 6 weeks. Lochia alba is rich in epithelial cells, white blood cells, fat, and bacteria.
Additionally, it’s important to assess the amount of lochia on the perineal pad every 60 minutes. A stain on the perineal pad that is less than 2.5 centimeters or 1 inch refers to a scant amount of lochia; less than 10 centimeters or 4 inches to a light amount; and finally, less than 15 centimeters or 6 inches refers to a moderate amount of lochia.
On the other hand, if there’s a complete saturation of the perineal pad in 60 minutes, that’s called heavy lochia. On the other hand, complete saturation of the perineal pad in 15 minutes is called excessive lochia. Irregularities in the duration, quality, and amount of lochia can be signs of an infection or uterine subinvolution where the uterus fails to return to its pre-pregnancy state.
Next, let’s take a look at the cervix. As the baby passes through the cervix, cervical trauma can occur, resulting in edema, bruises, and lacerations. After delivery, the internal os of the cervix fully closes, while the external os remains slightly open at about 2-3 centimeters at 2 to 3 days post-delivery. By the end of the first week, it narrows to less than 1 centimeter, and appears as a transverse slit.
The baby also causes trauma to the vaginal walls, which results in edema and lacerations. After delivery, the vagina loses folds and ridges of the vaginal walls called vaginal rugae, but they start to reappear 3 to 4 weeks after delivery. At 6 weeks after delivery, the vagina reaches a near pre-pregnant size.
Now, moving on to cardiovascular changes. After delivery, the blood that used to supply the uterus returns to systemic circulation, causing a transient increase in cardiac output that eventually returns to the prelabor values one hour after delivery.
Plasma volume also decreases after delivery. First, there’s a normal delivery related blood loss, which is typically 200 to 500 mL for a vaginal delivery ,and 600 to 800 mL for a cesarean delivery. Also, aldosterone and oxytocin production decreases, thereby increasing diuresis and fluid loss through urine; and there’s increased diaphoresis or sweating. Together, these processes decrease the plasma volume and return it to the prepregnancy levels by 6 weeks postpartum.
Moreover, this also normalizes the hematocrit values and coagulation factor levels. This usually occurs over the next 4 to 6 weeks. However, during this period, clients remain in a hypercoagulable state and are at increased risk for thromboembolic events