Physiology of lactation: Nursing
1,163views
Physiology of lactation: Nursing
Exam 1
Exam 1
Notes
| PHYSIOLOGY OF LACTATION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| BREAST ANATOMY & PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
Transcript
Lactation describes the process of milk production and secretion from the breasts; and it also refers to the period of time during which the mother is breastfeeding.
Let’s start by reviewing the physiology of the breasts. The breasts contain mammary glands responsible for lactation in biological females. Mammary glands are made up of 12 to 20 lobes, each of them containing many smaller lobules. These smaller lobules have grape-like clusters of alveoli that contain mammary secretory epithelial cells, the milk producing cells of lactation. These alveoli, lobules and lobes are connected through a network of ducts called the lactiferous ducts and eventually form a unique lactiferous duct for each lobe which opens independently to the areola to drain the milk produced during lactation. Each lactiferous duct has a dilated portion deep to the areola called the lactiferous sinus in which there’s a small drop of milk that accumulates or remains in a nursing mother, which becomes expelled from the areola when compressed during feeding.
During pregnancy, the placenta releases progesterone, estrogen, and human placental lactogen, while the pituitary gland releases prolactin. Now, these hormones work together to promote the development of breast tissue by increasing the number and size of the alveoli and the development of the lactiferous ducts.
Prolactin also stimulates milk production and during the later stages of pregnancy, the breasts produce an early version of breast milk called colostrum which is a thick yellowish fluid rich in immune cells and antibodies and high in protein. However, during this stage, high levels of progesterone and estrogen inhibit significant milk production to prevent wasting milk before the baby is born.
When the baby is delivered and the placenta is removed, the level of progesterone and estrogen decrease and milk production ramps up. 2 to 5 days after birth, the breasts start producing larger quantities of transitional milk which is higher in fat and lactulose but contains less antibodies. Finally, after about 2 weeks, the breasts start to produce mature milk which contains more water initially, but fat content increases later on.
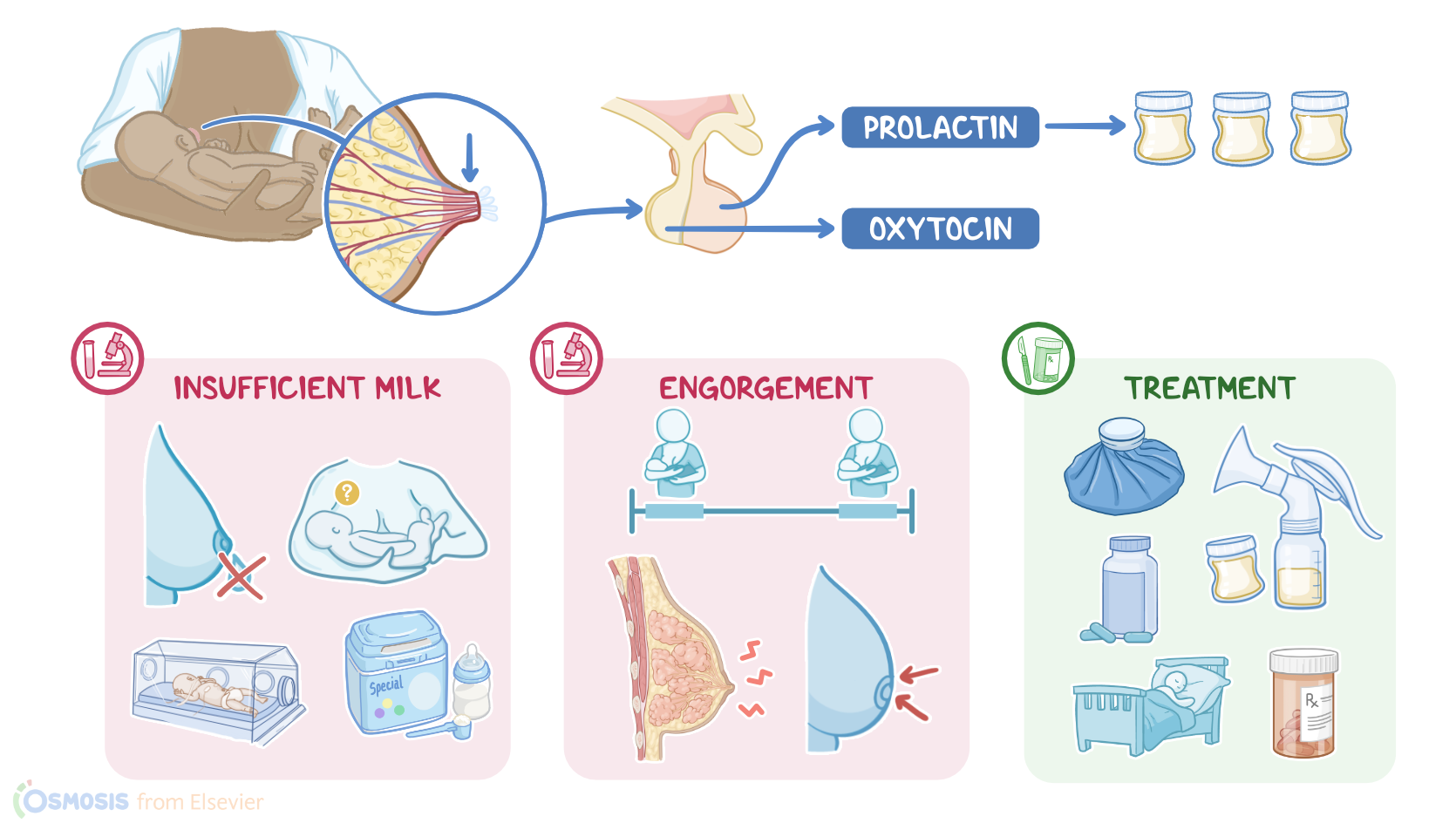
Now, milk secretion after birth is maintained by continuous stimulation of the nipple by the breast-feeding infant. This triggers the release of prolactin and oxytocin from the pituitary gland. Prolactin stimulates continued milk production, whereas oxytocin stimulates the contraction of smooth muscle cells around the ducts which causes the milk ejection or milk let-down reflex, causing milk secretion from the nipples. Finally, prolactin secretion during breastfeeding inhibits the hypothalamic-pituitary-ovarian axis that controls ovulation and menstruation, so typically, during breastfeeding the mother cannot get pregnant again.
Lactation ends after weaning the child, which causes decreased lactogenic hormones. This decrease signals cellular death, which results in shrinking or involution of the breasts where they return to the pre-pregnancy state.
Okay, now let’s look at some of the common issues of lactation, such as insufficient milk supply, breast engorgement, and mastitis.
Insufficient milk supply has many causes related to decreased stimulation of the breast. These include preterm delivery; ineffective infant suckling; infrequent or short feedings; and supplementing feedings with infant formula.
Sometimes, there can be a perceived insufficient milk supply during a baby’s growth spurt, when their feeding needs are temporarily increased, which can temporarily outpace the available milk supply.
Steps to ensure a good milk supply include breastfeeding frequently, as needed, which can be 8 to 12 times every 24 hours in the early weeks of life; avoiding supplementing feedings with formula unless necessary; and ensuring the baby has a good latch, so the breast can be effectively drained, which will then signal the body to produce more milk.
Sources
- " Breastfeeding: A guide for the medical profession (9th ed.) " Elsevier (2022)
- "Academy of Breastfeeding Medicine Clinical Protocol #36: The mastitis spectrum, revised 2022. , 17(5), 360-376. " Breastfeeding Medicine (2022)
- "Core Curriculum for Neonatal Intensive Care Nursing. ISBN 978-0323554190 " Elsevier Health Sciences (2020)
- "Seidel’s guide to physical examination (10th ed). ISBN 9780323761833 " Elsevier (2023)
- "Stability of Human-Milk oligosaccharide concentrations over 1 week of lactation and over 6 hours following a standard meal. ;152(12):2727-2733. " Journal of Nutrition (2022)
- "The impact of lactation education for nurses on infant breastfeeding rates during the early postnatal period. " Journal of Neonatal Nursing. (Published online August 1, 2023. )
- "Advanced Health Assessment & Clinical Diagnosis in Primary Care. ISBN 978-0323832069 " Elsevier (2023)
- "25 Years of Research in Human Lactation: From Discovery to Translation. 2021;13(9):3071. " Nutrients (Published 2021 Aug 31. )