Placenta previa: Nursing process (ADPIE)
1,459views
Notes
| PLACENTA PREVIA | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
30-year-old Sofia Ortiz, G5 T4 P0 A0 L4, is brought to the emergency department, or ED, by her sister with painless vaginal bleeding at 34 weeks of gestation.
She says that during the last 4 weeks she has experienced intermittent spotting and that she came to the ED because the bleeding has suddenly become bright red and much heavier.
Sofia has had routine prenatal care for all of her pregnancies, and each of her babies were delivered by cesarean section.
She has no known allergies, an uncomplicated medical history, and her only medications are prenatal vitamins.
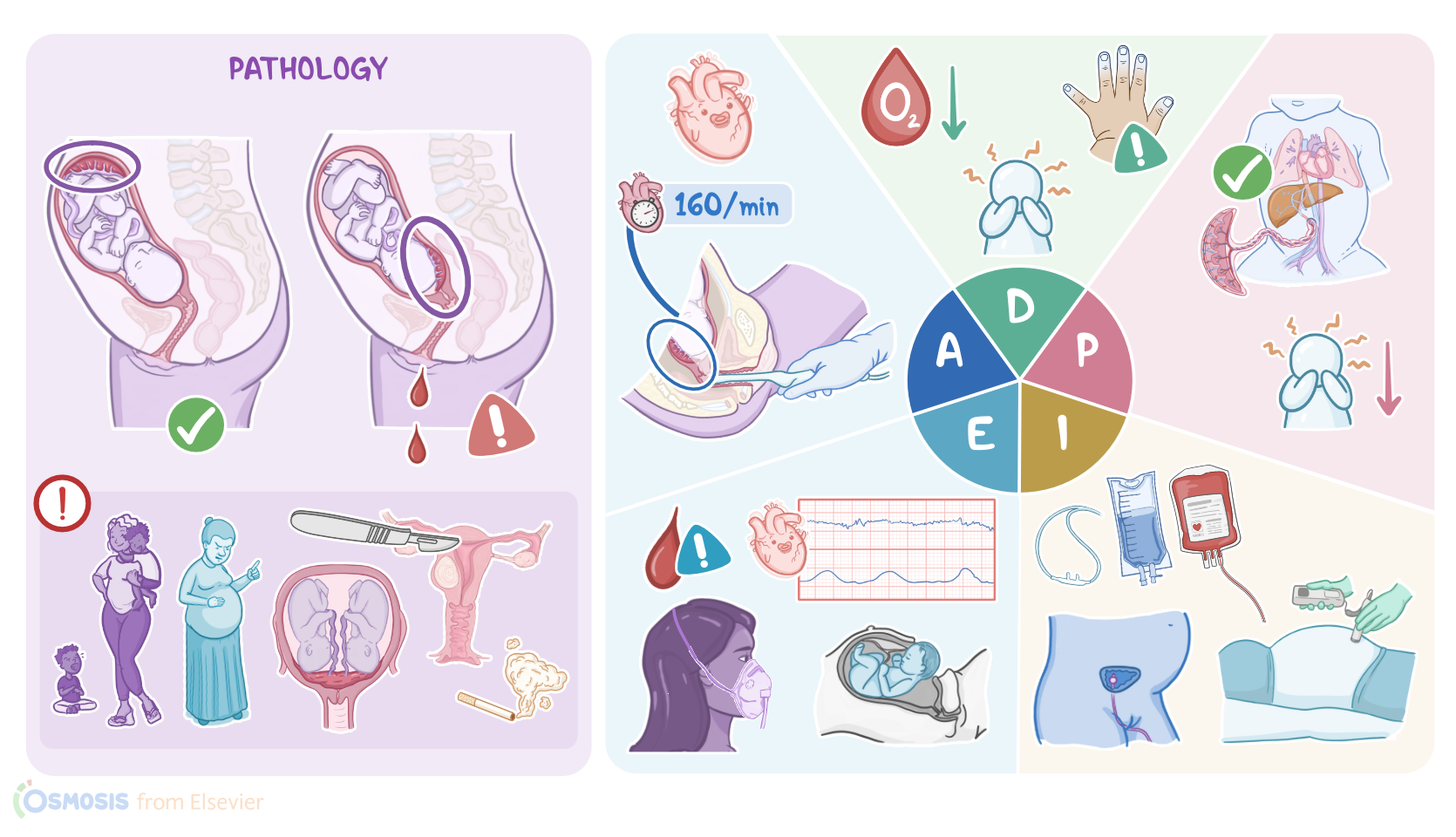
A focused assessment reveals active vaginal bleeding, an absence of uterine contractions and a baseline fetal heart rate, or FHR, of 150 beats per minute.
Sofia is transferred to the labor and delivery unit for monitoring. The placenta is a temporary organ that develops in the uterus during pregnancy, and it represents a lifeline connecti on between mother and fetus.
It provides oxygen and nutrients to a growing fetus, and also removes waste products from its blood.
Normally, the placenta implants in the upper uterus. Placenta previa occurs when the placenta implants in the lower part of the uterus and partially or completely covers the opening of the cervix, referred to as the cervical os.
Now, the exact reason why placenta previa occurs is still unknown, but there are some factors that can increase the risk for it.
The first risk factor is multiple gestation, in which the uterus must accommodate either more than one fetus with a larger placenta, or more than one placenta, each containing one fetus, which increases the risk of implantation near or over the cervical os.
Additionally, abnormalities of the uterus, such as uterine fibroids, can prevent the normal implantation of an embryo.
Also, previous uterine surgical interventions can cause uterine scarring and make the uterine lining less hospitable for implantation, which encourages implantation further down in the uterus.
The most important of these include previous cesarean birth and myomectomy, which is a surgical procedure used to remove uterine fibroids.
Other important procedures include multiple dilation and curettage procedures, which are performed to open the cervix and clear the uterine lining after a spontaneous or therapeutic abortion, or to remove abnormal uterine tissue.
Finally, individual risk factors include smoking, older maternal age, and multiparity, which refers to a history of two or more previous pregnancies.
Typical signs of placenta previa include sudden onset of bright red vaginal bleeding that is painless, and typically occurs after 20 weeks of gestation.
The amount of bleeding can vary, and it can increase during labor because of uterine contractions and cervical dilation.
Physical examination of clients with placenta previa reveals a soft, non-painful uterus.
The fetal heart rate, or FHR, can be normal initially, but as bleeding continues over time, decreased blood flow to the placenta may result in signs of fetal hypoxia and anemia.
Complications on the maternal end include hemorrhage, shock, and death.
On the fetal end, placenta previa can lead to serious complications such as intrauterine growth restriction, asphyxia, preterm delivery, and death.
Placenta previa is usually diagnosed with transvaginal or abdominal ultrasound, which typically reveals an abnormally positioned placenta.
A digital examination of the vagina is contraindicated if placenta previa is suspected because it can potentiate the bleeding. Instead, examination should be performed using a speculum.
In some clients, placenta previa is not recognized until cervical changes during labor cause bleeding.
For treatment, clients with placenta previa usually require hospitalization and close monitoring.