Rubeola (Measles): Nursing
Definitions & Key takeaways
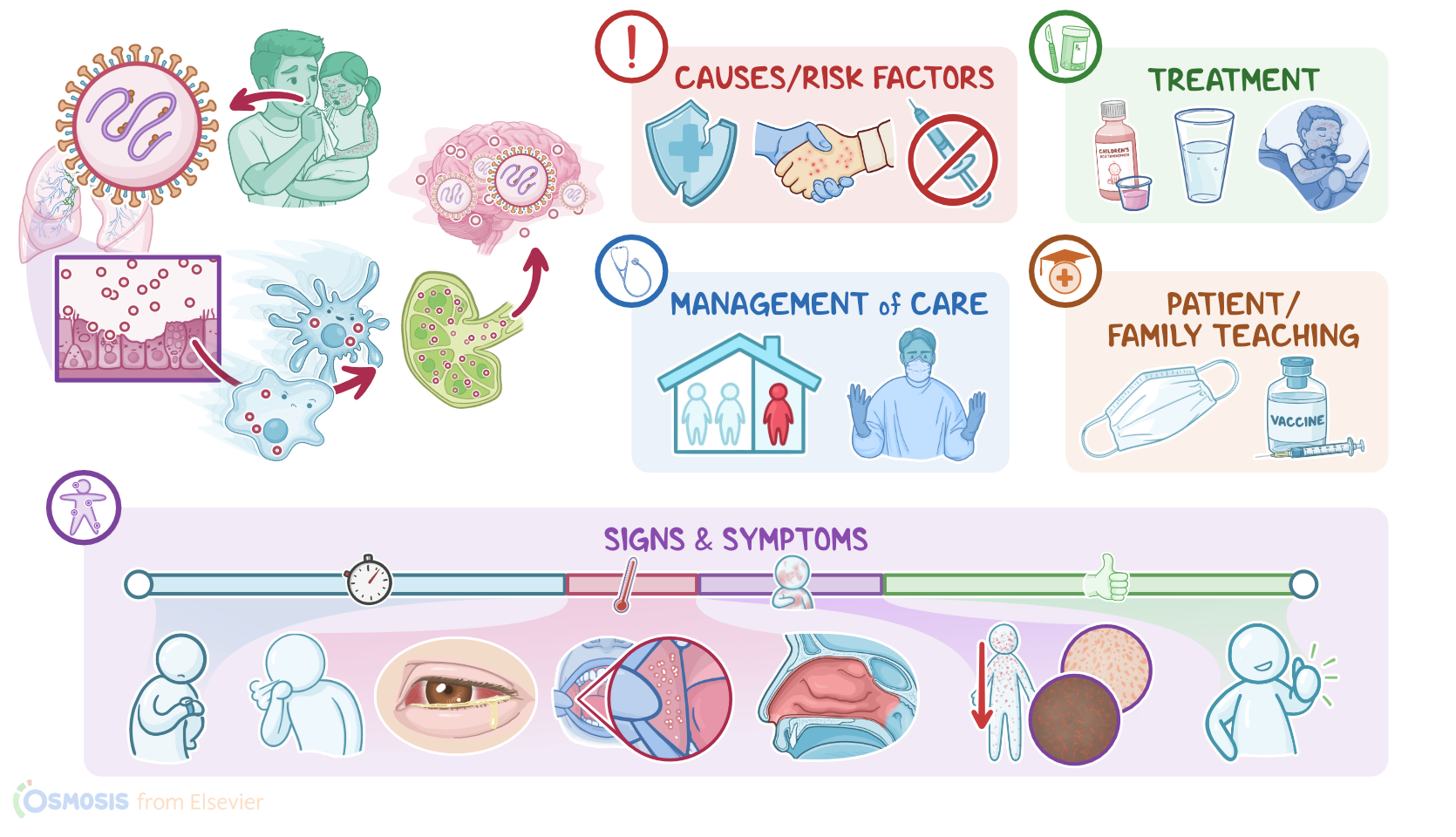
Rubeola, also known as measles, is a highly contagious viral infection caused by the measles virus. It spreads from person to person through coughing and sneezing. Risk factors for measles include immunodeficiency, being unvaccinated, vitamin A deficiency, pregnancy, and coming into contact with an infected person.
Symptoms of rubeola include cough, conjunctivitis, coryza, high fever, and a red rash that typically begins on the face and spreads to the rest of the body. Diagnosis of measles is typically based on the client's history and physical assessment, with the detection of measles-specific IgM antibodies for confirmation. Treatment for rubeola is supportive and may include bed rest, fluids, and fever-reducing medications. Vaccination is the best way to prevent rubeola.
Introduction0:00–0:31
Physiology0:31–1:21
Causes & risk factors1:21–1:46
Pathology1:46–4:10
Clinical manifestations4:10–5:13
Diagnosis5:13–5:33
Treatment5:33–6:11
Management and care6:11–8:01
General client and family teaching8:01–9:27
Review9:27–10:52
| RUBEOLA (MEASLES) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below