Sjögren syndrome: Nursing
Sjögren syndrome: Nursing
Medical Surgical
Medical Surgical
Notes
| SJOGREN SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
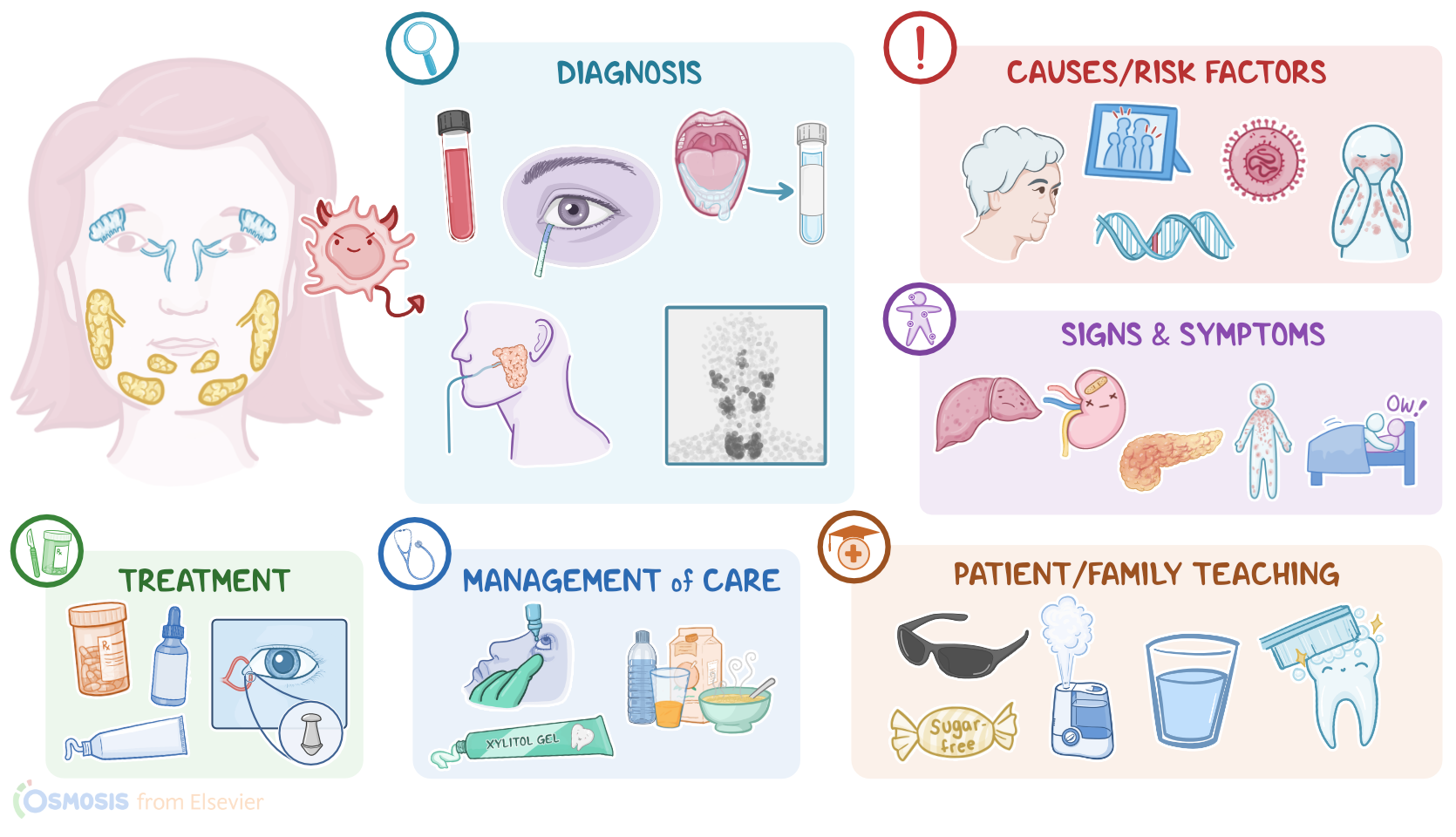
Sjogren syndrome is an autoimmune disease in which the immune system targets and attacks various exocrine glands, most commonly the lacrimal glands and the salivary glands.
Alright, now let’s quickly review the physiology of exocrine glands, which are found throughout body organs. These glands release various substances into a ductal system, which in turn carries these substances to an epithelial surface. Two particular examples of exocrine glands are salivary and lacrimal glands.
Now, there are three main pairs of salivary glands, called major salivary glands, which include the parotid, submandibular, and sublingual glands.
There are also a few smaller companions called minor salivary glands, which are sprinkled over the palate, lips, cheeks, tonsils, and tongue. When it comes to function, salivary glands secrete saliva into ducts that open in the oral cavity. Saliva contains enzymes that begin the digestion process, lubricates, and protects the mucosal surfaces of the mouth, in addition to preventing bacteria from forming dental cavities or caries.
On the other hand, lacrimal glands are paired exocrine glands located within the orbital cavity, just above the lateral angle of the eye. These glands secrete tears, which lubricate and nourish the surface of the eyes, help wash away debris, and act as a protective barrier against foreign particles, like pollen or dust.
The exact cause for Sjogren syndrome is unknown, but it seems to be related to both genetic and environmental factors. Sjogren syndrome typically affects clients over the age of 40, and risk factors include a family history of Sjogren syndrome, clients assigned female at birth, white or black race, as well as HLA genes that encode specific types of immune molecules, called HLA-DRW52, HLA-DQA1, or HLA-DQB1, which normally identify and bind to foreign molecules.
Environmental risk factors mainly include viral and bacterial infections of the exocrine glands, as well as being diagnosed with other autoimmune disorders, like rheumatoid arthritis or systemic lupus erythematosus. Okay, now the pathology of Sjogren syndrome starts with an environmental trigger, such as an infection, which damages the cells of the exocrine glands, mainly the salivary and lacrimal glands, and exposes their cell components to circulating immune cells.
At this point, the genetic components come in, meaning the client has HLA genes that cause their immune cells to recognize these antigens as foreign, which initiates an immune response that results in inflammation of the gland. Over time, the damaged gland tissue gets replaced by fibrous tissue, leading to reduced secretion.
Additionally, other exocrine glands can be involved, such as glands of the lungs, liver, pancreas, kidney, skin, and vagina.
Now, complications of Sjogren syndrome typically involve the eyes and the mouth and include corneal damage, dental cavities, and oral candidiasis. If other exocrine glands are also involved, Sjogren syndrome can lead to pneumonia, bronchitis, hepatitis, liver cirrhosis, primary biliary cirrhosis, pancreatitis, and renal damage, in addition to skin rashes, and vaginal dryness that may cause dyspareunia or pain during intercourse. Finally, these clients also have an increased risk of developing non-Hodgkin lymphoma, and thyroid disease.
Clinical manifestations of Sjogren syndrome vary depending on the exocrine gland affected. When the lacrimal gland is involved, clients can develop keratoconjunctivitis sicca, which is the inflammation and damage of the cornea and conjunctiva; this causes dryness of the eyes, or xerophthalmia, leading to blurring of vision, itching, redness, and burning of the eyes, as well as photosensitivity. When the salivary glands are involved, clients can experience xerostomia, or dryness of the mouth, as well as difficulty in tasting and swallowing, and cracks and fissures in the mouth. In any case, the affected glands can also become swollen, and in turn compress nearby structures like nerves, causing pain.
The diagnosis of Sjogren syndrome starts with the client’s history and physical assessment, followed by blood tests to detect autoantibodies associated with Sjogren syndrome, such as anti-Ro or SS-A antibodies, anti-La or SS-B antibodies, in addition to rheumatoid factor and antinuclear antibodies. Eye involvement can be tested by a Schirmer test, during which a small piece of filter paper is placed under the lower eyelid to measure tear production.
Other diagnostic tests include sialometry, which measures the saliva flow, as well as a sialogram, to visualize the salivary ducts, and a salivary scintigraphy, to assess the salivary glands’ function. Finally, diagnosis is confirmed with a labial salivary gland biopsy.
Treatment of Sjogren syndrome typically involves secretagogues, which are medications that increase the exocrine secretions, such as muscarinic agonists like pilocarpine and cevimeline. Some clients may also benefit from immunosuppressant medications like corticosteroids, or methotrexate; as well as antimalarials like hydroxychloroquine.
Clients with dry eyes may also benefit from preservative-free artificial tears and ophthalmic anti-inflammatory drops, such as cyclosporine. In severe cases, dry eyes can also be treated surgically with a procedure called surgical punctal occlusion, during which a punctal plug is inserted into the inner angle of the eye to keep the tears in the eyes for a longer time.
Finally, vaginal lubrication with a water-soluble product, such as K-Y Jelly, may help prevent discomfort during intercourse.
Okay, now let’s look at the nursing care you’ll provide to your client with Sjogren syndrome. Your priority nursing goal is to promote comfort.