Smallpox: Nursing
Smallpox: Nursing
Medical Surgical
Medical Surgical
Notes
| SMALLPOX | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Smallpox is a very contagious and potentially fatal viral disease caused by Variola virus and is usually associated with fever, malaise, headache and back pain followed by a characteristic rash. Thanks to vaccination, smallpox is the first human infectious disease that was successfully eradicated worldwide in 1980.
Let’s start by discussing the physiology of the immune response. It all begins in the bone marrow, where undifferentiated hematopoietic stem cells begin to differentiate into different types of white blood cells. Some of these cells migrate to the thymus where they become mature T cells, also known as T lymphocytes, which defend us against intracellular viruses, fungi, and tumor cells. Additionally, they are responsible for long-term immunity.
Now, after a foreign antigen enters the body, it runs into antigen-presenting cells, like macrophages and dendritic cells, by whom it is engulfed and digested into fragments. These antigen fragments are then presented on their surface and recognized by T helper cells, which help activate B cells to produce antibodies against that antigen. Next, these antibodies bind to any affected cell that expresses the antigen on its surface, eventually enabling natural killer or NK cells and cytotoxic T cells to easily recognize and destroy them. Furthermore, these natural killer cells enhance the inflammatory response by producing cytokines that recruit neutrophils, macrophages, and mast cells.
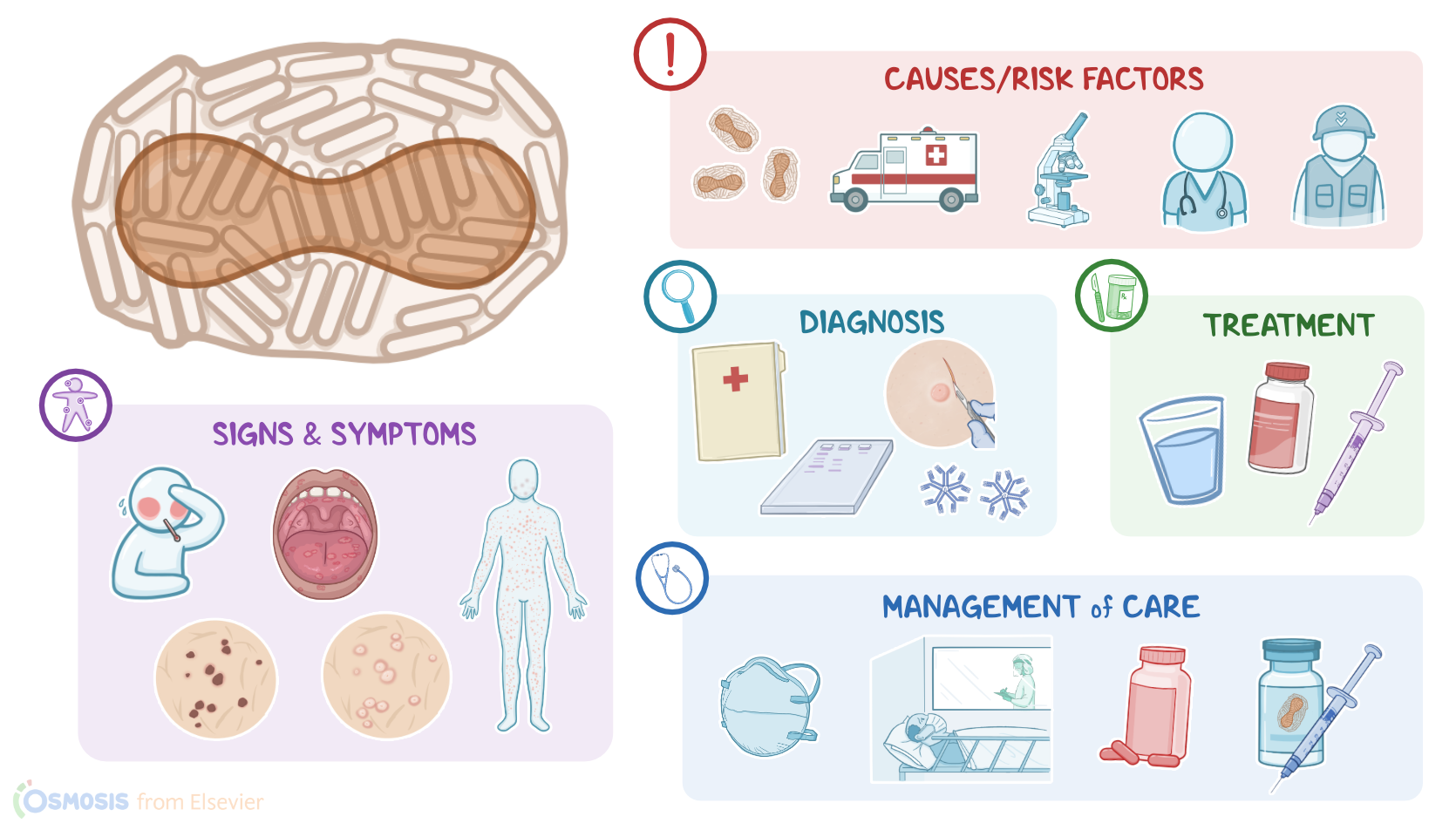
Okay, the cause of smallpox is Variola virus, which is a large DNA virus that belongs to the Orthopoxvirus genus and the Poxvirus family. Important risk factors for contracting smallpox, before it was eradicated, included close contact with an infected client or contaminated surfaces, infancy, older age and immunodeficiency. Nowadays, clients with occupational exposure, such as laboratory researchers that study Variola virus, health care workers, first responders, and military personnel can also be at risk. It’s important to know that even though smallpox has been eradicated, there is still a risk of the Variola virus being used as a potential bioweapon.
Moving on to pathology. Variola virus is an airborne virus, meaning it spreads via small virus-containing droplets that get flung in the air when an infected client coughs or sneezes. If another client breathes in these droplets, or they get in contact with infected surfaces and then touch their mouth, they can become infected. Clients can also become infected if they get in contact with the fluid from an infected client’s skin lesions, and then touch their own mouth.
In any case, once the virus enters the body, it invades epithelial cells in the nasopharynx and starts replicating in the cytoplasm, creating new viral particles that leave the cell. The virus then infects macrophages and dendritic cells, which carry it to regional lymph nodes where the virus replicates once again. From there, the virus enters blood vessels, causing what’s known as primary viremia, and spreads to other lymph nodes, as well as the spleen, bone marrow, and thymus. After replicating inside lymphoid organs, Variola virus enters blood vessels once again, causing secondary viremia, and making its way to other organs, such as the liver, kidneys, skin and mucosal membranes.
Now, complications of smallpox include secondary bacterial infections of the skin, bacterial pneumonia, encephalitis, osteomyelitis, viral arthritis and orchitis, as well as keratitis and corneal ulcerations which can lead to blindness. Rarely, smallpox can cause bone marrow suppression and heart failure. Also, as skin lesions heal, they can form residual pockmarks, which are deep and discolored scars.
Clinical manifestations of smallpox typically appear after an incubation period of 10 to 14 days and include high fever, severe headache, back pain, malaise and sometimes abdominal pain, vomiting and diarrhea. Two to four days later comes an enanthem, which is a rash on the mucous membranes of the tongue and palate. This is followed by the onset of an exanthem, or a red, macular rash that typically starts at the face, distal extremities, hands and soles of the feet, and then spreads to the trunk and proximal extremities. Over the course of 4 to 5 days, the lesions evolve from macules to papules to vesicles, filled with clear fluid, which can then turn into pus, giving rise to pustules. As these pustules pop open, the pus dries out and crusts form. An important characteristic of the smallpox rash is that all lesions are at the same stages of development at a time.
Diagnosis of smallpox typically begins with the client's history and physical assessment, followed by detection of smallpox-specific IgM antibodies. A PCR test can be used to detect viral DNA in the swabs of the oropharynx, conjunctiva, skin lesions, urine samples or organ biopsies. Additionally, biopsy of skin lesions can show Guarnieri bodies in the nuclei or cytoplasm of infected cells, which are aggregates of proteins produced by the virus as it replicates.
Key Takeaways
Smallpox is a highly contagious viral disease caused by the variola virus. Some of the risk factors for contracting smallpox before its eradication, included close contact with an infected client or contaminated surfaces, infancy, older age and immunodeficiency. Nowadays, clients with occupational exposure, such as laboratory researchers that study Variola virus, health care workers, first responders, and military personnel can also be at risk.
Infected people typically presents symptoms 10-14 days after exposure, which include high fever, headache, back pain, malaise, abdominal pain, vomiting and diarrhea, and after 1-4 days of these symptoms, a rash appears, which evolves to form macules to papules to vesicles, and eventually crusts.
Treatment usually involves supportive care as well as post-exposure prophylaxis to reduce the severity of the disease. Goals of nursing care include preventing disease transmission and providing supportive care. Client and family teaching is focused on learning about the disease and infection control measures.