Substance use disorder - Medications and illicit drugs: Nursing
Substance use disorder - Medications and illicit drugs: Nursing
Pharm
Pharm
Notes
| SUBSTANCE USE DISORDER - MEDICATIONS AND ILLICIT DRUGS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
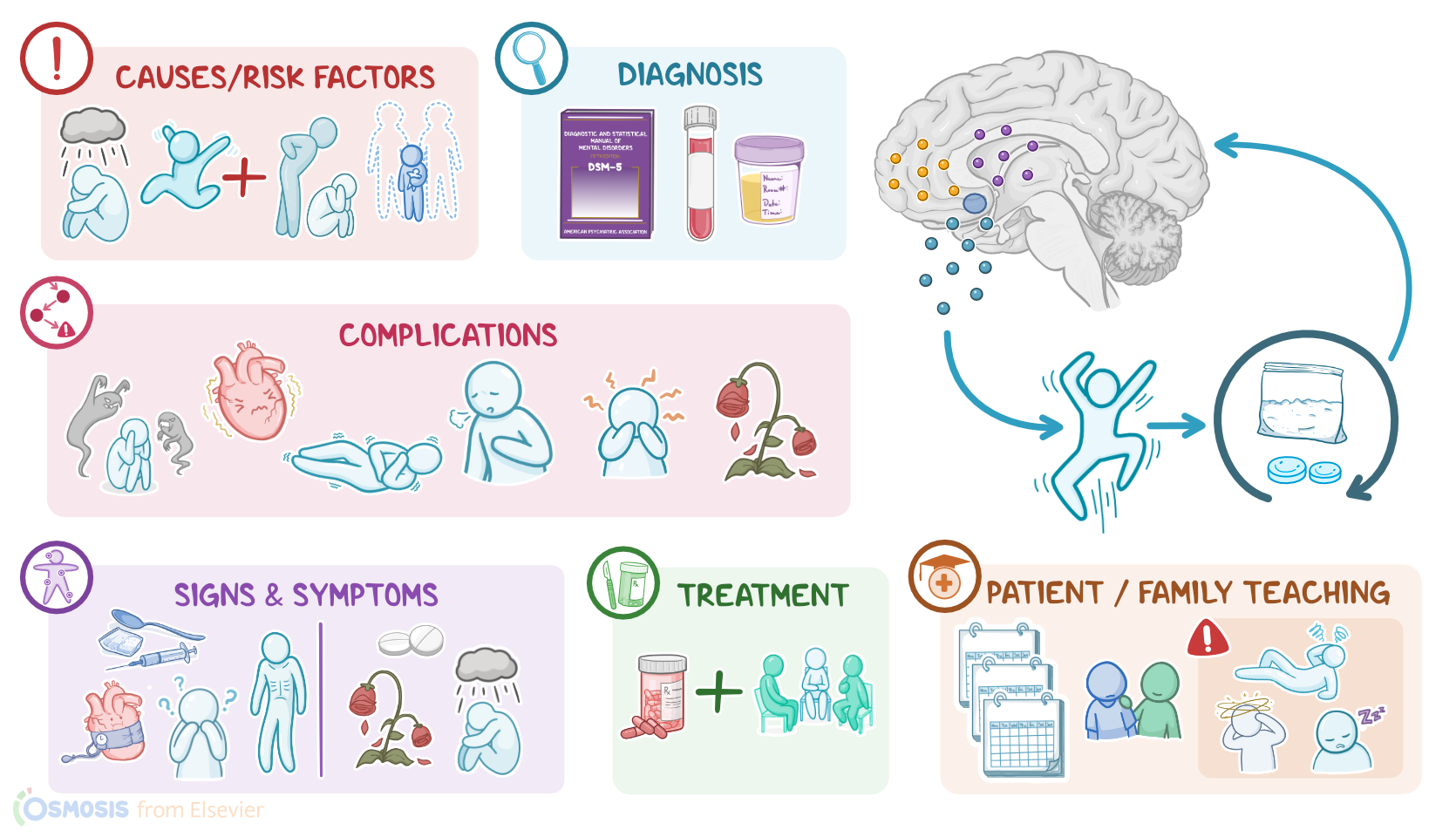
Substance use disorder is a condition in which an individual is unable to control their use of legal or illegal substances. Some of the most commonly used substances include stimulants like cocaine and methamphetamine, inhalants like paint remover and airplane glue, hallucinogens like cannabis and ecstasy, and finally, depressants like barbiturates, benzodiazepines, and opioids such as heroin or morphine. There are three different stages of substance use disorder: tolerance where an increased amount of the substance is needed to have the same effect; dependence where the substance is repeatedly used to avoid symptoms of withdrawal; and addiction where the substance use is recurrent, uncontrolled, and continued despite its harmful effects.
Okay, let’s quickly review the physiology of the brain’s reward center. Inside the brain are small molecules called neurotransmitters that are produced and used by neurons to communicate with each other. This communication happens when one neuron releases a neurotransmitter which then binds to the receptors of another neuron causing the neuron to react.
Now, the reward system of the brain governs pleasure and motivation. The center is the nucleus accumbens, a cluster of cells located near the hypothalamus. The primary neurotransmitter used in this system is dopamine which is released by the nucleus accumbens, causing a feeling of pleasure. These neurotransmitters stay in the junction between neurons for a while until they’re all taken back into the neuron via dopamine reuptake transporters, and the feelings of pleasure stops.
Now, there isn’t a single cause of substance use disorders, but rather it’s a multifactorial disease, meaning that there’s a combination of genetic predisposition and environmental risk factors and triggers. These include a family history of substance use disorder or having a mental health disorder like depression, ADHD, or PTSD. Certain experiences also put a client at high risk for developing a substance use disorder like using the substance at an early age or experiencing physical, sexual, or emotional abuse.
Okay, so let’s look at the pathology of substance use disorder. First, not everyone who uses a substance develops substance use disorder, for example someone who’s given morphine in the ER for kidney stones. A substance use disorder develops when long term use of a substance leads to severe physical, psychological, or social impairment in the client.
Now, everytime a substance is used, it causes intoxication, and this differs from substance to substance. However, what many of them have in common is they increase the level of dopamine either directly or indirectly. For example, cocaine can block the uptake of dopamine so it sticks around longer, while opioids turn off the neurons that inhibit dopamine release. This leads to the euphoric feeling which motivates the client to repeatedly use the substance.
Over time, neurons adapt to the chronic overexposure to dopamine by producing less and less dopamine or by reducing the number of dopamine receptors and becoming less sensitive to dopamine. Depending on the substance, the same process can also happen to other neurotransmitters like serotonin, GABA, and many others.
This lessens the effect of the substance so that the client needs to consume more and more of it to get the same euphoric feeling; and this is called tolerance. At this stage, if the client stops using the substance they may suffer withdrawal; and this is called dependence. Withdrawal symptoms can vary widely from substance to substance, for example, caffeine withdrawal might cause headaches, but barbiturate withdrawal can result in death. Finally, addiction happens when continued craving for the substance results in compulsive use, despite the harm it causes the client.
Each type of substance can also affect other parts of the body. Stimulants like nicotine, amphetamines, and cocaine can increase heart rate, cause vasoconstriction, and increase blood pressure. This can lead to ischemic damage to the heart, brain and kidneys. They also reduce a client’s appetite, leading to weight loss and malnutrition.
Hallucinogens like cannabis, PCP and LSD can cause distorted perception, hallucinations, agitation, memory problems, seizures, and ultimately a coma. Cannabis use has also been shown to increase the risk of developing mental disorders.
Finally, depressants like alcohol, opioids, benzodiazepines, and barbiturates can cause cardiac and central nervous system depression, which could lead to arrhythmias and coma. The most common cause of death from depressant use is respiratory depression due to decreased activity in the medulla; the part of the brain that regulates breathing.
Diagnosis of substance use disorder begins with the client’s history and physical assessment. Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria for substance use disorder. This includes impaired control like using more of the substance or using it longer than planned, intense desire to use or inability to cut down;
social impairment like ignoring responsibilities at work, home, or social situations, reducing time spent with family and friends, and problems with interpersonal relationships;
risky behavior like using the substance in dangerous situations like while driving, or continued use despite developing harmful medical conditions; and finally biological signs like dependence and withdrawal.
In addition, a blood or urine toxicology test is often performed to identify the substance used.
Treatment for substance use disorder usually involves a combination of psychotherapy and pharmacotherapy. There are several types of psychotherapy, including cognitive behavioral therapy, motivational enhancement therapy, group therapy such as support groups, and family therapy. These focus on teaching the client strategies to better cope with stress and social pressures, as well as to identify the thoughts, feelings, and behaviors that lead to substance use and create a plan to navigate triggers for use. In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Now, pharmacologic treatments have only been approved for opioid use disorder, where methadone, naltrexone, or a combination of buprenorphine and naloxone can be given to reduce symptoms and decrease cravings. Other medications can also be given, such as antiemetics, as well as alpha-2 adrenergic agonists to relieve autonomic symptoms like anxiety, diaphoresis, abdominal cramps, and diarrhea.
Now, more extensive support and treatment are required for acute substance intoxication. So, after making sure that the ABCs, or airway, breathing, and circulation are maintained, clients who are awake are typically induced to vomit and given activated charcoal to decrease gastrointestinal absorption. For clients who are in a coma, gastric lavage is often performed, after which activated charcoal is administered. In addition, it’s important to provide the right antidote like flumazenil for benzodiazepines and naloxone for opioids. Clients with stimulant intoxication typically also benefit from antipsychotics.