Testicular cancer: Nursing
Testicular cancer: Nursing
Oncology
Oncology
Notes
| TESTICULAR CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Testicular cancer is a rare form of cancer that can affect one or both testicles or testes. However, when it occurs, it’s usually in individuals assigned male at birth that are between 15 to 44 years old.
Let’s start with some anatomy and physiology. The testes are a pair of reproductive organs located inside the scrotum that hangs under the base of the penis, and are mainly responsible for producing testosterone and sperm cells. On a cross-section, each testicle has septa that partition it into lobules. Each lobule contains up to four seminiferous tubules, where sperm is synthesized from germ cells. These seminiferous tubules are lined up by specialized epithelial cells that contain Sertoli cells which envelopes and supplies nutrients to developing spermatocytes. Outside the tubules are Leydig cells, which produce and release testosterone.
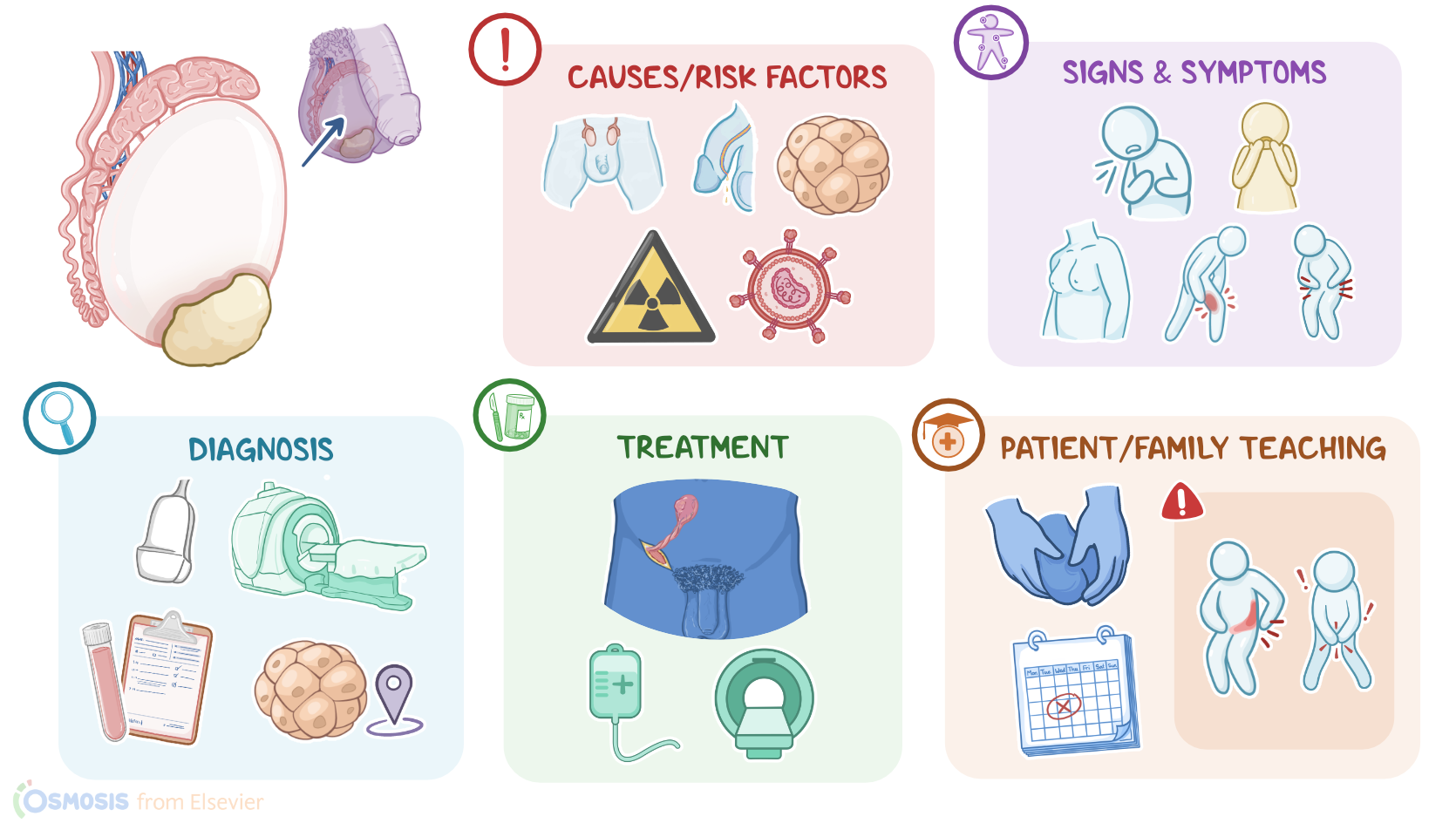
Although the exact cause behind testicular cancer is unknown, there are risk factors that can contribute to the development of testicular cancer. Such risk factors include Klinefelter syndrome; cryptorchidism, which means undescended testes; hypospadias, which is when the urethra opens underneath the tip of the penis; as well as having a past history of testicular anomalies, cancer, or radiation in the genital area; having HIV or AIDS; frequent marijuana use; and maternal exposure to pesticides or exogenous estrogen during pregnancy.
Now, when it comes to pathology, testicular tumors occur when cells in the testicle start to divide uncontrollably, and the end result is either a benign or a malignant tumor. Malignant tumor cells can spread to nearby tissue and even to other organs via the bloodstream or lymphatic system. The most common type of metastases are to the abdominal lymph nodes; but distant metastases to the lungs, liver, bones and brain can also occur. Now, based on the type of testicular cells that are involved, testicular cancers are broadly classified into two groups. First, there are germ cell tumors, which account for more than 95% of testicular cancers, and include seminomas, yolk-sac tumors, teratomas, choriocarcinoma and embryonal carcinomas. The second group includes non-germ cell tumors like Sertoli cell tumors and Leydig cell tumors.
Testicular cancer most often presents as a unilateral non-tender, firm and painless lump in the scrotum. Sometimes a sharp or dull pain can be felt in both testicles and lower abdomen. Other symptoms can be due to abnormal hormone secretion which can happen with any testicular cancer. Germinal cell tumors often produce human chorionic gonadotropin, or hCG, and it could cause gynecomastia, meaning the overdevelopment of breast tissue in individuals assigned male at birth. For non-germ cell tumors, Leydig cell tumors typically produce androgens like testosterone which can cause alopecia or male pattern baldness, and estrogen which can also cause gynecomastia. Sertoli cell tumors are more likely to produce estrogen so it also causes gynecomastia.
Signs of metastases depend on their localization. For example, lung metastases can cause dyspnea or coughing; liver metastases can cause jaundice, hepatomegaly and right upper quadrant pain ; bone metastases can cause bone pain; and brain metastases can cause neurological manifestations like headaches, impaired movement or sensation, poor coordination, difficulty speaking, or seizures.
Diagnosis starts with the client’s history and physical assessment. A scrotal ultrasound can help differentiate the testicular mass from cysts, and mark the size and border of the mass. Laboratory tests can reveal increased serum tumor markers like hCG; alpha-fetoprotein or AFP; and lactate dehydrogenase or LDH, as well as testosterone or estrogen in the case of hormone secreting tumors. A chest X-ray, as well as a CT or MRI scan of chest, abdomen and pelvis can be done to look for evidence of metastasis. With liver metastases, a comprehensive metabolic panel or CMP, can show increased liver enzymes like ALT and AST, as well as high bilirubin levels.
Staging depends on the size and location of the tumor, if it’s spread to any lymph nodes, if there’s any metastasis, and the levels of serum tumor markers. Finally, an inguinal orchiectomy, meaning the surgical removal of the whole testicle through the inguinal canal, is performed to make the final diagnosis and is also part of the treatment.
Treatment of testicular cancer can involve surgery, chemotherapy, and radiotherapy. An inguinal orchiectomy is usually the procedure of choice. After removal, a pathological work up or biopsy can be done to determine the histologic type of the tumor. Chemotherapy and radiotherapy can be done after surgery if the tumor has spread. Measuring levels of hCG, AFP and LDH before and after procedures can be useful in assessing the effects of the therapy and potential relapses.
Key Takeaways
Testicular cancers are malignant tumors that form in one or both testes. The cause is unknown, but risk factors include pre-existing conditions such as Klinefelter syndrome, cryptorchidism, hypospadias, history of testicular abnormalities, radiation of the genital area, HIV or AIDS, marijuana use, or maternal use of pesticides.
Major types of testicular cancer include germ-cell testicular cancer and non-germ-cell testicular cancer. Germ cell testicular cancers come from germ cells that normally develop into sperm. Common symptoms include a unilateral, non-tender, firm, and painless lump in the scrotum, dull or sharp pain in the testes and hormonal symptoms like gynecomastia. When metastasis occurs there could also be symptoms like jaundice, back pain, bone pain, and respiratory distress. Treatment involves surgery, sometimes in combination with chemotherapy, and radiotherapy.
Nursing management of care focuses on managing the effects of treatment, monitoring for metastasis, and providing psychosocial support. Client and family teaching focuses on learning about the planned treatment and the importance of testicular self-examination.