
Each week, Osmosis shares a USMLE® Step 1-style practice question to test your knowledge of medical topics. Today’s case involves a 60-year-old man with a seizure. The man dies two days later. Can you figure out the cause?
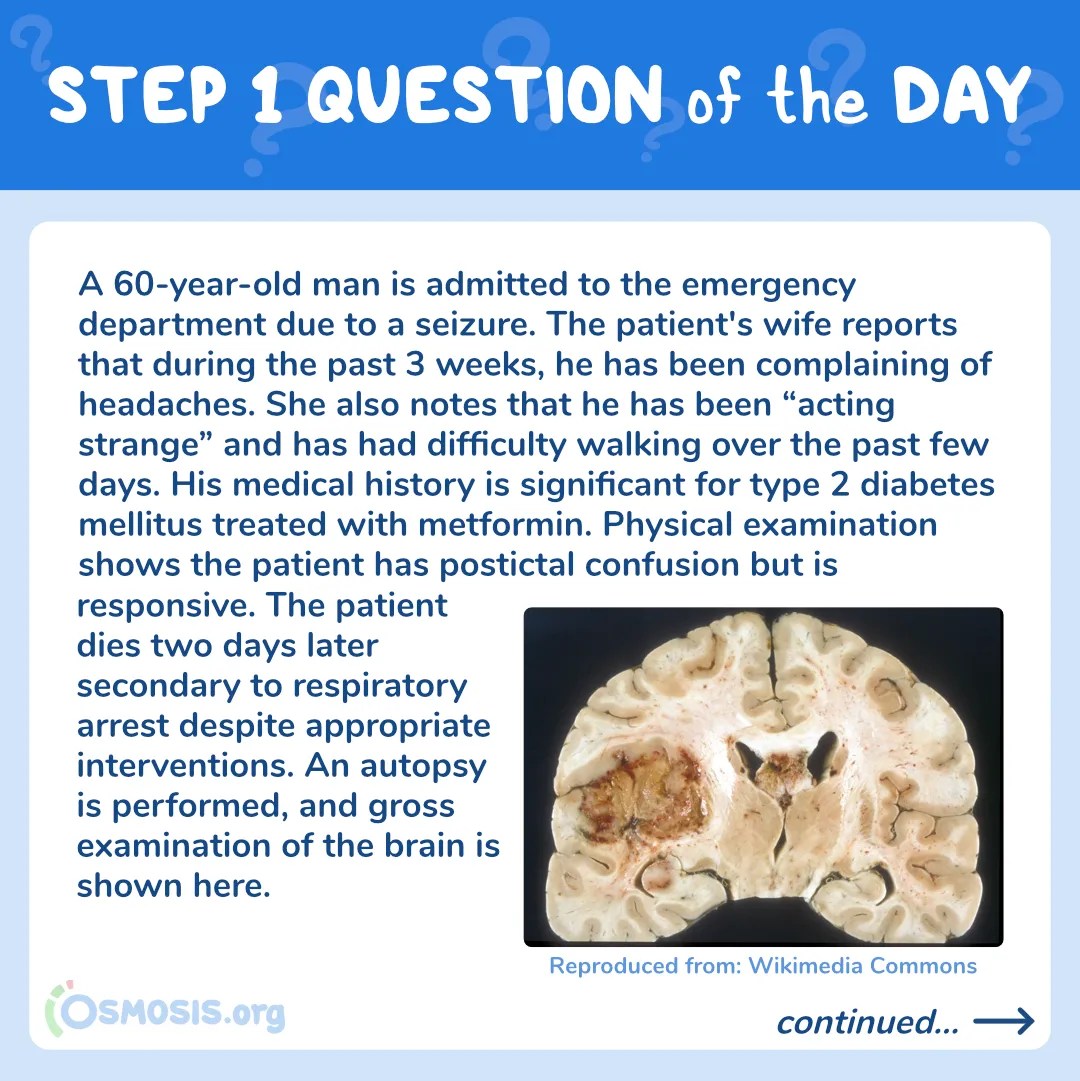
A 60-year-old man is admitted to the emergency department due to a seizure. The patient’s wife reports that during the past 3 weeks, he has been complaining of headaches. She also notes that he has been “acting strange” and has had difficulty walking over the past few days. His medical history is significant for type 2 diabetes mellitus treated with metformin. Physical examination shows the patient has postictal confusion but is responsive. The patient dies two days later secondary to respiratory arrest despite appropriate interventions. An autopsy is performed, and gross examination of the brain is shown below:

Reproduced by: Wikimedia Commons
Histopathological examination of this patient’s lesion is most likely to show which of the following findings?
A. Concentrically arranged spindle cells in a whorled pattern with areas of calcifications
B. Hypercellular areas of spindle cells alternating with hypocellular myxoid areas
C. Large abnormal lymphocytes infiltrating perivascular spaces
D. Thin-walled capillaries with minimal intervening parenchyma
E. Pleomorphic tumor cells surrounding an area of central necrosis
Scroll down to find the answer!
→ Reinforce your understanding with more self-assessment items on Osmosis.
The correct answer to today’s USMLE® Step 1 Question is…
E. Pleomorphic tumor cells surrounding an area of central necrosis
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
The incorrect answers to today’s USMLE® Step 1 Question are…
A. Concentrically arranged spindle cells in a whorled pattern with areas of calcifications
Incorrect: These histological findings are consistent with meningiomas, which are common, typically benign tumors of arachnoid cell origin. Meningiomas are extra-axial (external to brain parenchyma) and may have a dural attachment. This patient autopsy shows an intra-axial tumor with central necrosis and hemorrhage, which favors the diagnosis of glioblastoma multiforme.
B. Hypercellular areas of spindle cells alternating with hypocellular myxoid areas
Incorrect: These histological findings are consistent with a Schwannoma, a tumor of Schwann cell origin. It commonly arises at the cerebellopontine angle, involving both cranial nerves VII and VIII, but it can occur along any peripheral nerve. Patients present with sensorineural hearing loss and tinnitus. This patient’s autopsy shows an intra-axial tumor in the cerebral hemispheres with central necrosis, which favors the diagnosis of glioblastoma multiforme.
C. Large abnormal lymphocytes infiltrating perivascular spaces
Incorrect: These findings are consistent with primary central nervous system lymphoma, a rare form of non-Hodgkin lymphoma seen most commonly in immunocompromised patients (e.g. HIV). Typical locations include the corpus callosum, periventricular white matter, and basal ganglia, presenting as either solitary or multiple lesions. This patient is immunocompetent with a characteristic lesion on autopsy, which favors another diagnosis.
D. Thin-walled capillaries with minimal intervening parenchyma
Incorrect: These histological findings are consistent with hemangioblastoma, a tumor of blood vessel origin. These tumors most often arise in the cerebellum and are associated with von Hippel-Lindau syndrome. This patient’s tumor morphology and location favors another diagnosis.
Main Explanation
This patient’s presentation (seizures associated with progressive headache, weakness, and personality changes occurring rapidly over the course of several weeks), in addition to the characteristic gross morphology seen on autopsy, is consistent with the diagnosis of glioblastoma multiforme (GBM).
GBM, or grade IV astrocytoma (astrocyte origin), is a highly malignant primary brain tumor with an approximately 1-year median survival. On histology, the tumor stains positive for glial fibrillary acidic protein (GFAP) and is characterized by “pseudopalisading” pleomorphic tumor cells bordering central areas of necrosis, hemorrhage, and/or microvascular proliferation. On gross morphology, tumors are often large, poorly defined, and have areas of necrosis and hemorrhage. On imaging, GBM is seen as a ring-enhancing lesion, because the contrast-enhancing tumor cells form a ring to surround the necrotic center, which does not take up contrast. The tumor can cross the corpus callosum, leading to a midline shift and causing a mass effect (“butterfly glioma”).
Major Takeaway
Glioblastoma multiforme is a common, highly malignant primary brain tumor with poor survival rates. On histopathology, it stains positive for glial fibrillary acidic protein (GFAP) and shows “pseudopalisading” pleomorphic tumor cells that form a ring around a central area of necrosis and hemorrhage.
References
Chang SM, Parney IF, Huang W, et al. Patterns of care for adults with newly diagnosed malignant glioma. JAMA. 2005;293(5):557‐564. doi:10.1001/jama.293.5.557
Valentinis L, Tuniz F, Valent F, et al. Headache attributed to intracranial tumours: a prospective cohort study. Cephalalgia. 2010;30(4):389‐398. doi:10.1111/j.1468-2982.2009.01970.x
Reuss DE, Sahm F, Schrimpf D, et al. ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol. 2015;129(1):133‐146. doi:10.1007/s00401-014-1370-3
Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg. 1988;68(6):835‐853. doi:10.3171/jns.1988.68.6.0835
_________________________
Want more USMLE® Step 1 practice questions? Try Osmosis today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning with us.

The United States Medical Licensing Examination (USMLE®) is a joint program of the Federation of State Medical Boards (FSMB®) and National Board of Medical Examiners (NBME®). Osmosis is not affiliated with NBME nor FSMB.
Leave a Reply