Anthrax: Nursing
Anthrax: Nursing
Respiratory System
Respiratory System
Notes
| ANTHRAX | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Anthrax is a zoonotic disease caused by Bacillus anthracis, which is a Gram positive, rod-shaped bacterium, which primarily enters the body through the skin, lungs, gastrointestinal tract, and through direct injection. Infection with Bacillus anthracis is associated with high mortality.
Now, first, let’s cover some basic physiology of the skin. The most superficial layer of the skin is the epidermis, which is in close contact with the outside world and primarily serves as a protection from foreign pathogens. Next up is the dermis, which is made up of connective tissue that contains blood vessels, lymphatics, nerve endings, as well as immune cells, like macrophages and dendritic cells. These cells represent innate immunity and they are first on the scene when a pathogen breaches the skin and enters the body. Finally, the deepest layer of the skin is called hypodermis and is primarily made up of adipose tissue.
Now, let’s switch our focus to the anatomy of the respiratory tract. When we breathe in, the air flows through the nasal and oral cavity into the pharynx and larynx, down into the trachea or windpipe. Next, the trachea splits into two main stem bronchi that enter the lungs and branch into smaller bronchi, which further give rise to smaller conducting and respiratory bronchioles, and finally alveolar ducts. Alveolar ducts open up into alveolar sacs, which are small grape-like groups of alveoli where the gas exchange takes place. Within the alveoli, there are immune cells called alveolar macrophages, which help clean the alveolar space from foreign substances but also fight pathogens that make it to the lungs.
Finally, let’s cover the basic histology of the gastrointestinal tract, starting with the outermost layer, which is called the adventitia or serosa. Next up are the muscularis externa and the submucosa; and finally, the innermost layer is called the mucosa. Moreover, the mucosa secretes mucus, digestive enzymes, and absorbs nutrients from the gastrointestinal lumen.
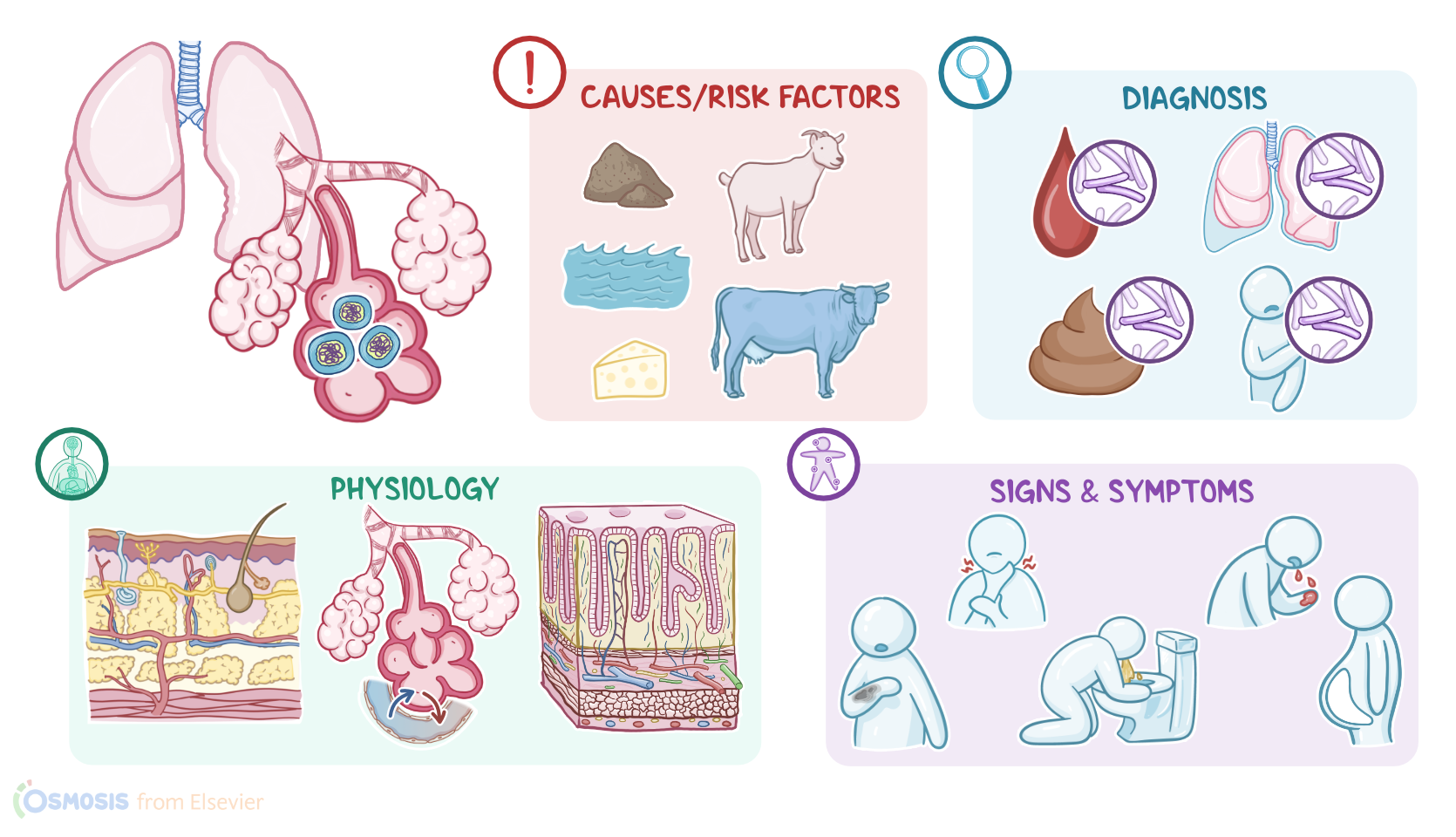
The cause of anthrax is Bacillus anthracis, which primarily infects domestic animals, such as sheep, cattle, and goats. The bacteria can undergo endosporulation and develop spores, which are the most resistant forms of the bacteria. Spores can contaminate soil, food, water, as well as animal products.
Important risk factors for Bacillus anthracis infection include eating undercooked meat; living in rural or agricultural areas; and working with animals or animal products, so those most at risk are farmers, veterinary workers, but also other individuals who come in close contact with animal wool, skin, and hides. It also has been used as a bioterrorism agent.
Now, the pathology of anthrax varies, depending on the organ system that is infected. First, let’s start with cutaneous anthrax which occurs when spores of Bacillus anthracis come in contact with an open wound or other break in the skin. Here, spores germinate and give rise to the active bacteria, which produce the anthrax toxin. The anthrax toxin locally damages the surrounding tissue, eventually causing skin ulceration and edema.
On the other hand, in inhalation anthrax, the person inhales spores and they eventually end up within the lung alveoli. Next, alveolar macrophages engulf the spores and transport them to regional mediastinal lymph nodes. But when macrophages fail to contain the infection, the spores germinate, produce the anthrax toxin, and cause local tissue destruction, including hemorrhagic mediastinitis.
Then there’s gastrointestinal anthrax, which most commonly occurs when a person ingests undercooked meat that contains spores. Once in the gastrointestinal tract, spores once again start to germinate, producing active bacteria that secrete the anthrax toxin. As a result, there’s local destruction of the gastrointestinal mucosa that can eventually lead to ulcerations and bleeding.
Finally, injection anthrax occurs when an individual injects spore-contaminated heroin. The anthrax spores are injected directly into the body, and once toxin is produced, it leads to local tissue damage as well as gastrointestinal or central nervous system manifestations.
Complications of Bacillus anthracis infection include hemorrhagic mediastinitis, gastrointestinal bleeding, pleural effusion, and respiratory failure, meningitis, septic shock, and even death.
Now, clinical manifestations of cutaneous anthrax usually appear 1 to 10 days after the inoculation with spores. The most important clinical feature is a pruritic papular lesion that typically progresses to a painless ulcer surrounded by small vesicles and blisters. Over time, the lesion becomes necrotic with a black center. At this point, it’s called eschar and it’s surrounded by non-pitting edema. As the lesion heals, the eschar dries and sheds off over the next 2 weeks.
On the other hand, clinical manifestations of inhalation anthrax typically occur 1 to 6 days after the inhalation of spores. This type of anthrax is also known as woolsorter's disease, and it’s characterized by nonspecific clinical manifestations, such as fever, malaise, nausea, and vomiting.
On the flip side, respiratory features usually include dyspnea and nonproductive cough, as well as stridor from an obstructed airway. In severe cases, a client might become hypoxic or cough up blood.
Clients with gastrointestinal anthrax usually become symptomatic 1 to 7 days after the ingestion of spores. Bacillus anthracis can affect any part of the gastrointestinal system, from the mouth to the rectum. Clients with oropharyngeal anthrax typically present with regional lymphadenopathy and dysphagia; while clients with intestinal anthrax, usually complain of nausea, vomiting, diarrhea, as well as fever.
In severe cases, intestinal anthrax can cause acute clinical manifestations, such as bloody diarrhea, hematemesis, and ascites, which refers to the accumulation of fluid in the peritoneal cavity. Finally, injection anthrax typically presents with local tissue edema, cellulitis and tissue necrosis, but can progress to shock, meningitis, or cerebral bleeds.
Diagnosis of anthrax usually starts with the client’s history, physical assessment, and routine blood test like a CBC and blood chemistries. Imaging methods, such as X-ray and CT scan, could show pleural effusions or a widened mediastinum.
The diagnosis is confirmed by detecting the presence of the bacteria in the blood, pleural fluid, stool, or at the site of infection. This can be done through microscopy of infected fluid, such as skin lesions or cerebrospinal fluid; as well as microbial cultures or PCR testing.
Sources
- "Medical-Surgical Nursing" Elsevier (2020)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Saunders (2019)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Saunders (2016)
- "Study Guide for the Core Curriculum for Oncology Nursing" Saunders (2019)
- "What Is Anthrax?" Pathogens (2022)
- "Current Status and Trends in Prophylaxis and Management of Anthrax Disease" Pathogens (2020)
- "Anthrax toxin component, Protective Antigen, protects insects from bacterial infections" PLOS Pathogens (2020)