Arterial embolism: Nursing
Notes
| ARTERIAL EMBOLISM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
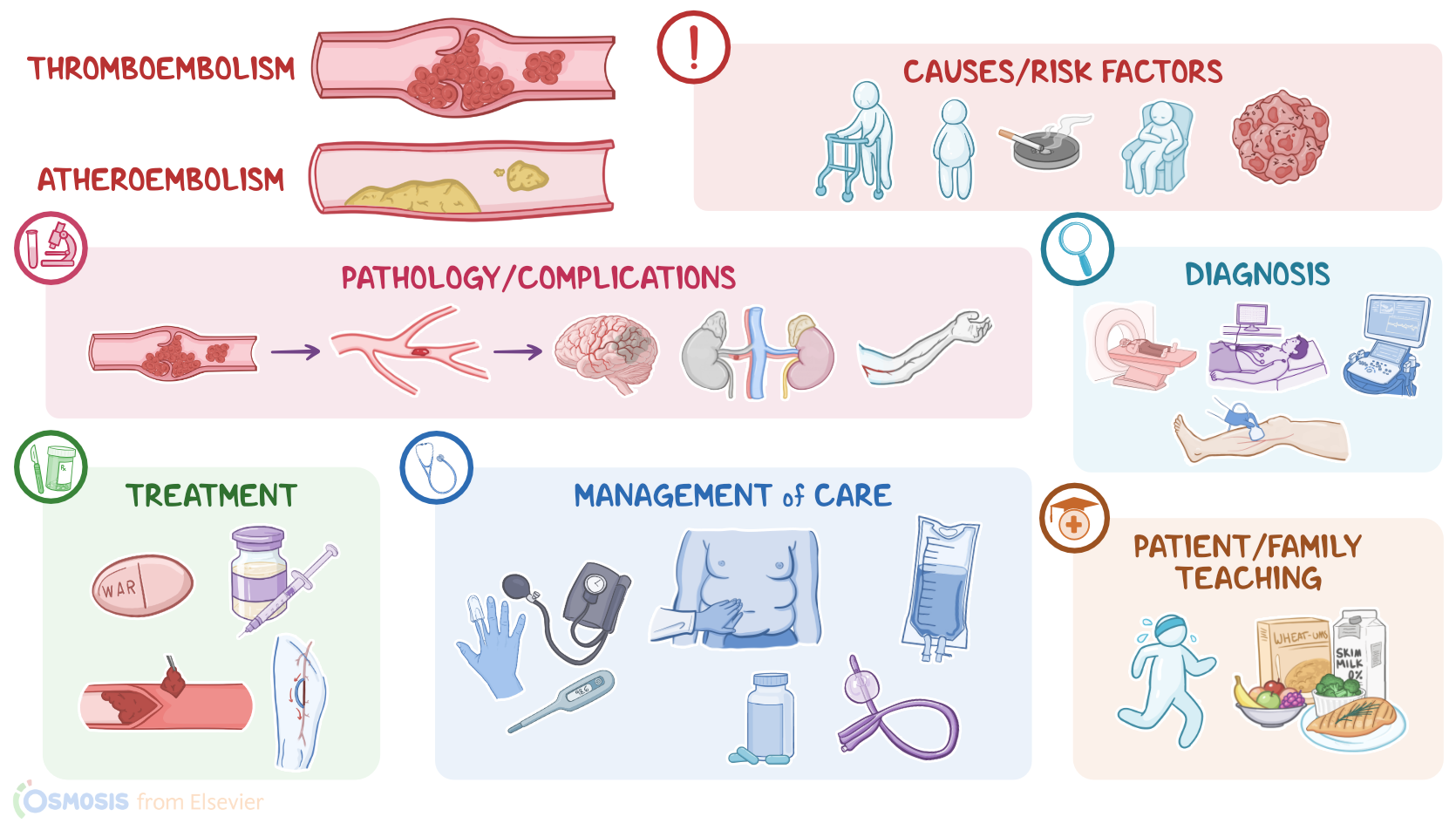
Arterial embolism occurs when some material lodges in an artery, subsequently causing a sudden interruption of arterial blood supply to parts distal to the occlusion. The most common types of arterial embolism include thromboembolism, which occurs when a blood clot, or thrombus, breaks loose, becoming an embolus; and atheroembolism, which occurs when cholesterol crystals from an arterial plaque break loose and enter the circulation.
Alright, let’s cover some basics of physiology. There are three major types of blood vessels: arteries, veins, and capillaries. Normally, blood flows from large arteries into medium and then small arteries called arterioles, which in turn deliver oxygen-rich blood into a network of capillaries, called the capillary bed. Here, oxygen and nutrients pass to tissue cells, which will then return carbon dioxide and wastes back into the capillary bed. These capillaries will then merge to form the smallest veins, called the venules. Eventually, these venules converge to form small veins, which then drain into medium superficial veins. Next, these superficial veins drain blood into medium deep veins, which continue to converge, forming large veins that eventually drain back into the right side of the heart. From here, venous blood goes into the lungs, where it gets oxygenated.
Now, let's zoom in and take a closer look at the arterial wall, which consists of three layers: from outside in, there’s tunica externa or the adventitia layer, which has loose connective tissue; then tunica media or the middle layer, which contains some elastic tissue and smooth muscle that allow the artery to dilate or constrict in response to local conditions; and finally the endothelium, which consists of a single layer of endothelial cells on top of a layer of connective tissue, called lamina propria. The endothelial cells maintain blood flow by preventing blood cells from reaching the underlying lamina propria. Additionally, endothelial cells express small molecules such as heparin sulfate and prostacyclin, which help prevent blood coagulation. So, if their continuity is disrupted, blood cells may come up against coagulation factors in the lamina propria. This initiates a coagulation cascade that leads to the formation of a blood clot, which in turn blocks the blood flow.
Now, causes of arterial embolism can be either internal causes, such as atherosclerotic plaque, thrombosis or clots, fat from broken bones, and cancer tissue; or external causes, like air from a surgical procedure, amniotic fluid or fetal debris during birth, and even foreign objects, like bullets.
Now, atherosclerotic plaque refers to the accumulation of cholesterol and other lipids on the inner surface of a blood vessel, which can affect important arteries, such as aortic arch and carotids. Part of the plaque can break off forming a cholesterol emboli that travels down the artery and eventually causes an obstruction.
Now, emboli can also form in the heart. When there’s an arrhythmia like atrial fibrillation, blood can’t be pumped out properly so it pools in the left atria and increases the risk of forming a blood clot. Blood clots can also form on damaged heart valves or prosthetic heart valves. With endocarditis, bacterial infection of a heart valve can also trigger the formation of a blood clot that can turn into an embolus. Finally there’s paradoxical embolism. There is when an embolus that forms in a vein travels back to the right side of the heart, but gets to the left side of the heart through a ventricular septal defect. Once in the left ventricle, it gets pumped into the systemic circulation and obstructs an artery.
Now, risk factors for arterial embolism include individual risk factors, such as prior history of thromboembolism, advanced age, and pregnancy, as well as lifestyle risk factors, like smoking, obesity, and sedentary lifestyle. There are also conditions associated with an increased risk of arterial embolism, including clotting disorders, atherosclerosis, cardiac arrhythmias, valvular heart diseases, and endocarditis, as well as cancers. Risk factors that increase the risk of atherosclerosis like high cholesterol, smoking, and hypertension also increase the likelihood of arterial embolism. Finally, other risk factors include trauma, surgical interventions, prolonged bed rest and immobility, central venous catheters, and estrogen therapy.
Now, once a blood clot, cholesterol crystals, or any other substance, such as air, fat, or a foreign object, enters the systemic circulation, it becomes an embolus. From there an embolus can lodge where arteries branch or narrow. This results in mechanical obstruction of the artery and decreases blood flow to the area, causing tissue ischemia distal to the occlusion. When tissue necrosis occurs it is also known as infarction, which is irreversible damage due to a lack of oxygen and nutrients.
Now, let’s cover important complications of arterial embolism. In the brain, the blood clot can cause an embolic stroke; in kidneys, renal artery embolism; while the occlusion of intestinal arterial blood vessels, can result in mesenteric artery embolism. Blood clots can also reach extremities and obstruct the arterial blood supply of the limbs.
Alright, switching gears and moving on to clinical manifestations of arterial embolism, which are primarily based on the location of the affected artery and the part of the body that it supplies. First, let’s focus on clinical manifestations of embolic stroke, which vary depending on the artery that is blocked and the part of the brain that is affected. Most commonly, these clients present with ataxia, limb weakness, and loss of motor and sensory functions. Additionally, they might present with facial drooping; dysarthria, which is difficult or unclear speech; and dysphagia, or difficulty in swallowing.
On the other hand, clients with renal artery embolism usually present with flank pain, fever, and hematuria, as well as nausea and vomiting; while in clients with mesenteric artery embolism, there’s a periumbilical abdominal pain accompanied by nausea and vomiting.
Arterial embolism of the extremities usually present with 6 Ps: Pain; Pallor, or loss of color; Pulselessness, or absence of the pulse in the affected limb; Poikilothermia, which is the inability of the affected part to regulate tissue temperature; Paresthesia, which is often described as a burning sensation; and Paralysis, which is a late sign of arterial embolism. Moreover, if not recognized on time, arterial embolism of extremities can eventually lead to nerve damage, or even tissue necrosis and gangrene.