Autism spectrum disorder (ASD): Nursing
Introduction0:00–0:34
Autism spectrum disorder, or ASD, is a neurodevelopmental disorder that manifests during infancy or early childhood and is associated with social communication and interaction deficits, as well as restrictive or repetitive behavior, interests, and activities, which can interfere with how a client functions independently in society.
Many previously separate disorders like Autistic disorder and Asperger disorder now fall under ASD. First, let’s look at childhood developmental milestones, which are skills or behaviors that most infants are able to perform at a specific age.
Developmental milestones0:34–3:14
These milestones can be divided into social, communication, cognitive, and movement. Social milestones include starting to smile at 2 months of age.
By 4 months, they can copy facial expressions. At 6 months they can recognize familiar faces and enjoy playing with others.
At 1 year, they enjoy playing games like peekaboo and show fear with strangers. By 2 years of age, they enjoy playing with other children, show more independence, and start being more defiant, the so-called terrible 2s.
Communication-wise, at 2 months, infants can coo and say “ga” and will respond to sounds. By 4 months, they can babble and try to copy sounds they hear.
By 6 months, they start stringing together vowels like ooh-ahh-ehh and respond to their own name. At 1 year, they can respond to simple requests like “come”, say simple words like mama and dada, and use simple gestures like waving bye bye.
By 2 years of age, they can point to the correct object when named, and say sentences with 2 to 4 words. Next, regarding cognitive development, at 2 months they start following moving objects with their eyes, and pay more attention to faces.
By 4 months they’ll watch moving toys and reach for them, and by 6 months they’ll start showing curiosity about objects they can see.
By 1 year, they can use simple objects correctly like brushing their hair with a comb, and they will experiment with different objects by banging, shaking, or throwing them.
By 2 years, they can follow 2 step instructions like pick up the ball and throw it in the basket, they can sort objects by categories such as color, shape, and size, and name familiar items like bird, cat, house.
Finally, when it comes to motor development, at 2 months infants should be able to hold their head up. At 4 months they should be able to hold their head steady without support, roll over from their tummy to their back, hold a toy in their hand, and press down with their leg when standing on a hard surface.
By 6 months, they can roll front to back and back to front, and sit without support. By 1 year, they can stand on their own, and walk while holding onto objects.
By 2 years, they can kick a ball, run, stand on their tiptoes, and walk up and down stairs. Now, the exact cause of autism spectrum disorder is still unknown, but it’s believed to be linked with mutations in certain genes that regulate normal brain development.
Causes & risk factors3:14–4:15
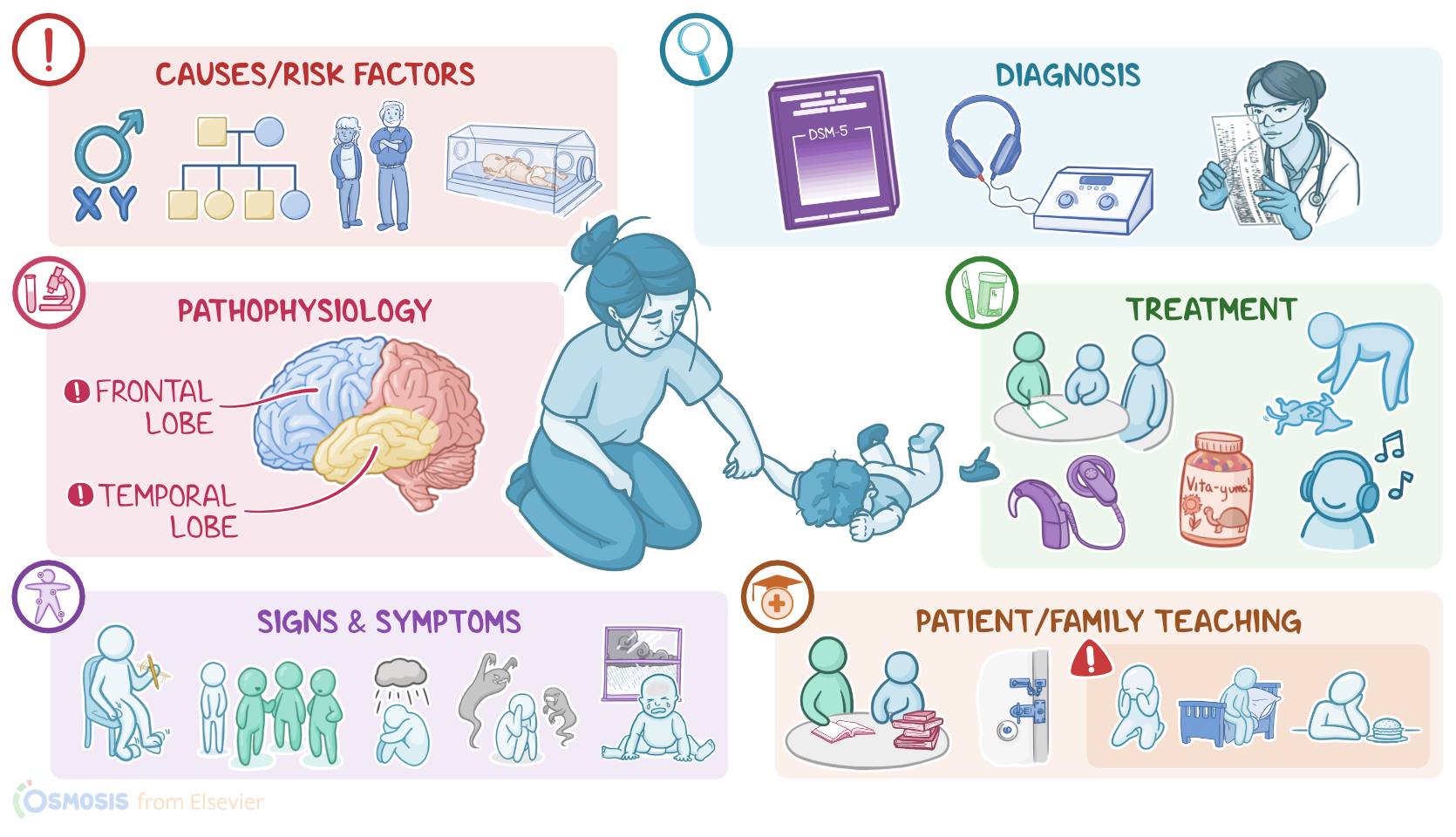
Important risk factors that have been associated with the development of autism spectrum disorder are mostly non-modifiable, and include being assigned male at birth, family history of autism spectrum disorder, older parental age, and prematurity.
Clients with certain genetic syndromes, such as fragile X syndrome, tuberous sclerosis, Rett syndrome, and Down syndrome, are also at an increased risk for developing autism spectrum disorder.
Modifiable risk factors include maternal infections during pregnancy, as well as prenatal exposure to toxic agents, such as certain antiepileptic medications.
However, no link has been found between ASD and MMR vaccination. Okay, the exact pathophysiology of autism spectrum disorder is still not fully understood, but it looks like there’s abnormal development in certain regions of the brain like the frontal and temporal lobes, which are responsible for regulating social and communication behaviors.Clinical manifestations of autism spectrum disorder usually appear before 2 years of age, but they might also appear later in life.
Pathophysiology4:15–4:35
Clinical manifestations4:35–8:20
Children with ASD often have several delayed developmental milestones, especially social and communication milestones. However, there’s a lot of variability.
Some children develop early milestones normally but fail to progress to later milestones. For example, they might start babbling at month 4, but they can’t say simple words like mama and dada by age one.
Others might develop some milestones normally, but miss others. So at the age of 2, they might show more independence, but refuse to play with others.
In addition to missing milestones, clients with ASD develop social and communication deficits. There are three main types of social and communication deficits.
First is deficits in social-emotional reciprocity, ranging from a difficulty with normal back-and-forth conversation to completely failing to initiate and respond to social interactions.
This is often made worse by the fact that many clients with autism spectrum disorder also experience hearing impairment.
Second is deficits in nonverbal communication like difficulty coordinating speech with eye contact. And third is deficits in developing, maintaining, and understanding social relationships, which includes adjusting behavior to suit a specific context, to difficulties with making and keeping friends.
In addition to these deficits, clients have restrictive and repetitive behaviors, interests, and activities. These include stereotyped or repetitive motor movements like eye twitches, use of objects, or speech.
They might also have highly restricted, fixated interests like a strong attachment to candles. And finally, they show hyper- or hypo reactivity to specific sensory stimulation, like being indifferent to pain or getting extremely upset by the sound of rain.Clients with autism spectrum disorder might exhibit one or more of these deficits, and vary in how severe the deficit is.
Based on this, they can be grouped into three functional levels. Level one clients are functional and verbal but have a hard time establishing relationships.
They are often perceived as weird or eccentric due to their behavior, or lazy and insecure because they might be late to meet their developmental milestones.
Level two clients have more prominent social difficulties, may only use simple sentences to express their needs and have obvious repetitive and odd behaviors.
Level three clients have severe functional limitations, are usually non verbal or may only use a few words and require constant care and support.In any case, a common comorbid condition for ASD is epilepsy, which develops typically during early childhood or adolescence.
Complications of ASD include dependency on others to function normally, which puts additional pressure and stress on the whole family.
Clients with problems establishing social relationships with others, might experience social isolation, learning difficulties, and problems with school and finding jobs.
Children with ASD can also be commonly bullied and victimized by their peers. Finally, it's important to remember clients with ASD are at a higher risk for developing depression, anxiety and psychotic disorders.
Okay, diagnosis of autism spectrum disorder is based on the client’s history and physical assessment. Primary care providers, or PCPs, usually perform screening of children using Modified Checklist for Autism in Toddlers-Revised which is a questionnaire for parents about their child’s behavior.
Diagnosis8:20–9:52
It is performed at 18 months of age with a follow up at 24 and 30 months of age. If autism spectrum disorder is suspected, the client is then referred to a specialist, such as a child's psychiatrist, that can establish the diagnosis based on the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria.
This is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a condition.
Now, based on the DSM-5 criteria, to diagnose autism spectrum disorder the client must have persistent defects in social and emotional reciprocity, non-verbal communication and relationship development.
Additionally, they must have at least two out of four types of restrictive and repetitive behaviors, including stereotyped or repetitive motor movements; rigid adherence to routines; restricted interests with abnormally high focus; or abnormal reactivity to sensory stimuli.
Additionally, hearing tests might be needed to look for hearing impairment. Finally, genetic testing is sometimes also performed to identify associated genetic syndromes.
That being said, there’s no cure for autism spectrum disorder, so supportive treatment should begin as early as possible, that is specifically and carefully tailored to each client, and aims at helping clients maximize quality of life and functional independence.
Treatment9:52–11:17
It mainly consists of non-pharmacological therapy, including behavioral and communication therapy, where clients can learn how to cope with various social situations; intensive educational therapy, especially in a highly structured educational environments; family training, so that families can understand the needs of their children and learn how to play and interact with them; speech therapy, to help the client improve their communication skills; physical therapy, to improve client's independence; and occupational therapy, to improve everyday activities.
In addition, some clients may benefit from alternative therapies, including nutritional supplements, vitamins, restrictive diet, music and art therapy, pet and horse riding therapy and sensory integration techniques.In difficult cases, medications can be used to control some symptoms, such as antidepressants, like SSRIs, for anxiety, antipsychotics for aggressive behavior and stimulants for controlling hyperactivity.
FInally, hearing impairment services can also help improve problems with hearing. Okay, let’s take a look at the care you would provide for a child with ASD.
Your goals or care are to provide a therapeutic care environment, promote effective communication, maintain safety, and support your client’s caregivers.
Management and care11:17–13:31
Begin planning your care by assessing their individual needs. Ask your client’s caregivers about their child’s sensitivity to stimuli, and take steps to decrease external stimuli by providing care in a quiet room, that has dimming lights, and is away from noisy alarms and other auditory stimuli.
Also, avoid fast movements or rushing when providing care by planning on taking extra time for assessments and interventions, and taking breaks as needed.
Next, focus on communicating with your client. Observe them closely and ask their caregivers about their child’s specific communication needs.
Be sure to speak with a calm voice, and communicate strategically using short, simple sentences such as “First drink water, then TV time” or “Does your belly hurt?” Depending on their individual needs, incorporate simple non-verbal strategies such as picture boards or simple signs for needs like pain, thirst, or hunger.
Lastly, ensure your client has a referral for speech therapy.To keep your client safe, ask the child’s caregivers about any triggers, how to tell if they are becoming escalated, and how to calm them.
Then, structure your care to avoid situations that could result in frustration and aggressive behavior. For example, if your client has difficulty with change, develop a routine and stick with it to the extent possible.
Or, if your client engages in certain repetitive, soothing movements, allow them to the extent that it doesn’t hinder care.
Lastly, complete a safety assessment to keep the client’s care environment free of objects that could be used to harm themselves or others.
Report to the healthcare provider if your client develops any new or worsening symptoms such as a sudden refusal to communicate; increased anxiety or aggressiveness, or attempts to harm themselves or others.Finally, remember to provide support for your client’s caregivers, as they are often fatigued and worried about their child.
If needed, arrange family counseling and discuss the need for respite care. Be sure to offer positive reinforcement and active listening.
General client and family teaching13:31–15:03
Provide resources for support groups to help them develop an alliance with other caregivers of children with ASD.Now, when providing teaching for your client and their caregivers, begin by reinforcing their understanding of the disorder and the available supportive treatments.
Encourage them to work closely with the healthcare team to support their child attain their highest level of functioning.
Next, review strategies to promote their child’s development. Talk about ways to provide a safe, structured environment and a routine that aligns with their child's specific needs.
Emphasize the need for maintaining a safe environment to reduce the risk of behaviors that can be self-injurious or have the potential to hurt others.
This can include keeping potentially harmful items out of their child’s reach; or if the child tends to wander, using locks, gates, window or door alarms, as well as having their child wear identification bracelets or Global Positioning System Tracking devices.Finally, instruct them to contact the healthcare provider right away if their child develops any new or worsening symptoms, including unusual sadness, decreased appetite, difficulty sleeping, irritability, or unusual aggressiveness.Autism spectrum disorder, or ASD, is a neurodevelopmental disorder that is associated with social, communication, and interaction deficits, as well as restrictive or repetitive behavior, interests, and activities, which can interfere with how a client functions independently in society.
The cause of autism is still unknown, although it's believed to be linked with mutations in certain genes that regulate normal brain development.
Review15:03–17:32
Risk factors include being assigned male at birth, family history of autism, older parental age, and prematurity. The exact pathophysiology of autism is not fully understood, but it seems to be a problem with brain development in the frontal and temporal lobes.
Complications of autism include job difficulties, dependency on others to live normally, social problems, and being bullied.
Clinical manifestations are usually present before 2 years of age, and can become more apparent later in life. They vary widely, and can include social and communication deficits, along with restrictive and repetitive behaviors.
Autism is diagnosed based on the client’s history and physical assessment. Screenings can include the Modified Checklist for Autism in Toddlers-Revised, or M-CHAT-R at 18 months of age.
If autism is suspected, the client will be referred to a specialist who will diagnose them based on diagnostic criteria.
For diagnosis, the client must have persistent defects in social and emotional reciprocity, non-verbal communication and relationship development, and at least two out of four types of restrictive and repetitive behaviors.Treatment should begin as early as possible, be tailored to the individual client, and aim to maximize the client’s quality of life and functional independence.
It can include behavioral and communication therapy, family training, speech therapy, physical therapy, and occupational therapy.
In severe cases, antidepressants like SSRIs, antipsychotics, or stimulants can be used if appropriate. Goals of nursing care include providing a therapeutic care environment, promoting communication, maintaining safety, and supporting the client’s caregivers.
Client and family teaching is focused on strategies for caring for the child at home and when to contact the healthcare provider.
and occupational therapy in severe cases, antidepressants, like ssris antipsychotics or stimulants can be used if appropriate goals of Nursing Care.
Include, providing a therapeutic care environment promoting, communication maintaining safety and supporting the clients caregivers client and family teaching is focused on strategies for caring for the child at home.
And went to contact the healthcare provider.
| AUSTISM SPECTRUM DISORDER (ASD) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| DEVELOPMENTAL MILESTONES |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below