Buerger disease: Nursing
Buerger disease: Nursing
Cardiovascular MedSurg
Cardiovascular MedSurg
Notes
| BUERGER DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
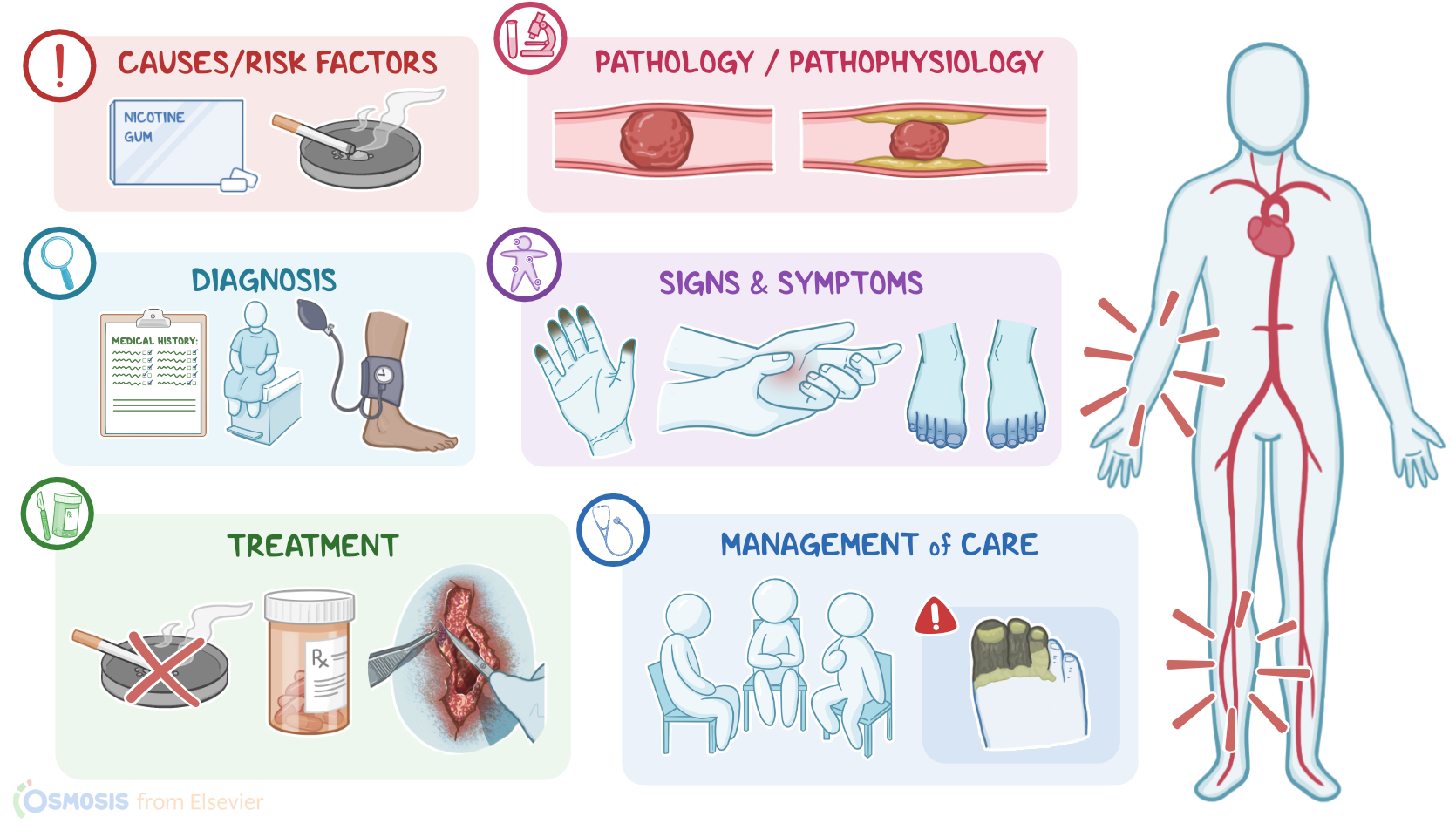
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Buerger disease, also called thromboangiitis obliterans, is a peripheral vascular condition characterized by inflammation of small and medium-sized arteries and veins of the extremities. This inflammation is recurrent, segmental, and non-atherosclerotic, meaning that it’s not caused by atherosclerosis.
All right, let’s go over some physiology. There are three major types of blood vessels: arteries, veins, and capillaries. Normally, blood flows from large arteries into medium and then small arteries called arterioles, which in turn, carry the blood to capillary beds. All arterial vessels have three layers: from outside in, there’s tunica externa or the adventitia layer, which has loose connective tissue; then the tunica media or the media layer, which contains some elastic tissue and smooth muscle that allow the arteriole to dilate or constrict in response to local conditions; and finally, the endothelium, which consists of a single layer of endothelial cells on top of a layer of connective tissue, called lamina propria.
The endothelial cells maintain blood flow by preventing blood cells from reaching the underlying lamina propria. If their continuity is disrupted, blood cells may come up against coagulation factors in the lamina propria. This initiates a coagulation cascade that leads to the formation of a blood clot, which in turn blocks the blood flow.
Now, the arterioles deliver oxygen-rich blood into a network of capillaries, called the capillary bed. Here, oxygen and nutrients pass to tissue cells, which will then return carbon dioxide and wastes back into the capillary bed. These capillaries will then merge to form the smallest veins, called the venules. The structure of these venules is similar to that of arterioles but with thinner walls that contain less smooth muscles. Eventually, these venules drain blood into medium veins, which then drain into large veins that deliver the blood straight back to the heart.
All right, now the exact cause of Buerger disease is still unknown, however the single most important risk factor is long-term tobacco use. Other risk factors include marijuana use, clients assigned male at birth, and age between 25 and 35, without other cardiovascular disease risk factors like hypertension, hyperlipidemia, and diabetes.
Now, the course of Buerger disease consists of two phases: acute and chronic. In the acute phase, an inflammatory thrombus forms within the walls of small and medium-sized blood vessels. At first, this thrombus is filled with immune cells, but later on, organization may occur, which describes the migration of more cells into the thrombus, like smooth muscle cells and fibroblasts.
As this thrombus matures and gets larger, the disease progresses into the chronic phase, which is characterized by vascular fibrosis, meaning proliferation of fibroblasts and collagen deposition. The enlarging thrombus and the resulting vascular fibrosis narrow the blood vessels, decreasing the blood flow to the tissues, and eventually causing tissue ischemia and death.
Clients with Buerger disease typically present with intermittent claudication, which is intermittent pain that most often affects the calf, but can also involve the foot, thigh, or even the arms, and is induced by exercise and relieved by rest. In cases of advanced disease, this pain may even come at rest, along with ulcers that result from the ischemia, called ischemic ulcerations.
Other signs and symptoms that may arise in the affected limb include paresthesia, as well as skin color and temperature changes. Some clients may also present with Raynaud phenomenon, meaning that when exposed to a trigger, such as emotional stress or exposure to cold temperatures, their fingers and toes turn white, then blue, and then red.
Additionally, clients with Buerger disease may have delayed capillary refill time, which indicates hypoperfusion of the involved tissue. In the most severe cases, the client could develop necrosis and gangrene.
Now, the diagnosis of Buerger disease is usually based mostly on history and physical assessment. Diagnostic tests may include an Allen test to assess the degree of arterial circulation to the client’s hands. This can be followed by the ankle–brachial index or ABI test to rule out peripheral artery disease. Finally, additional tests should focus on ruling out other unrelated conditions that may also present with intermittent claudication, such as thrombophilia, diabetic neuropathy, aneurysms of the popliteal artery, and autoimmune diseases, like scleroderma.
When treating a client with Buerger disease, the goals are to prevent ischemic tissue damage and improve quality of life. Initial treatment is typically focused on the complete cessation of tobacco, including nicotine replacement products, in addition to the complete cessation of marijuana use in any form. Avoiding triggers like cold exposure may also help prevent Raynaud phenomenon. If this is not enough, the client can be given analgesics for the pain, as well as medications that help induce vasodilation and improve blood flow to the extremities, such as calcium channel blockers, phosphodiesterase-5 inhibitors, or topical nitrates. Clients with infected ulcers may also require antibiotics.
Now, in severe refractory cases, surgical treatment options might be considered, such as lumbar sympathectomy. This is when surgery is performed to cut the sympathetic nerve fibers supplying the affected areas. This reduces leg pain associated with ischemia, and aids in the healing of ischemic ulcers. The next option is implanting a spinal cord stimulator, which is a small device that sends low electrical pulses to the spinal cord to reduce pain. Finally, necrotic areas may require surgical debridement or even amputation.
All right, now let’s look at the nursing care you will be providing a client with Buerger disease. Priority goals of care center on promoting blood flow to affected areas, preventing infection, and managing pain. Begin by assessing your client’s extremities, including blood pressure, distal pulses, capillary refill, skin color and sensation, and the presence of ulcers.