Cholecystitis: Nursing
2,302views
Cholecystitis: Nursing
Acute Final
Acute Final
Notes
| CHOLECYSTITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
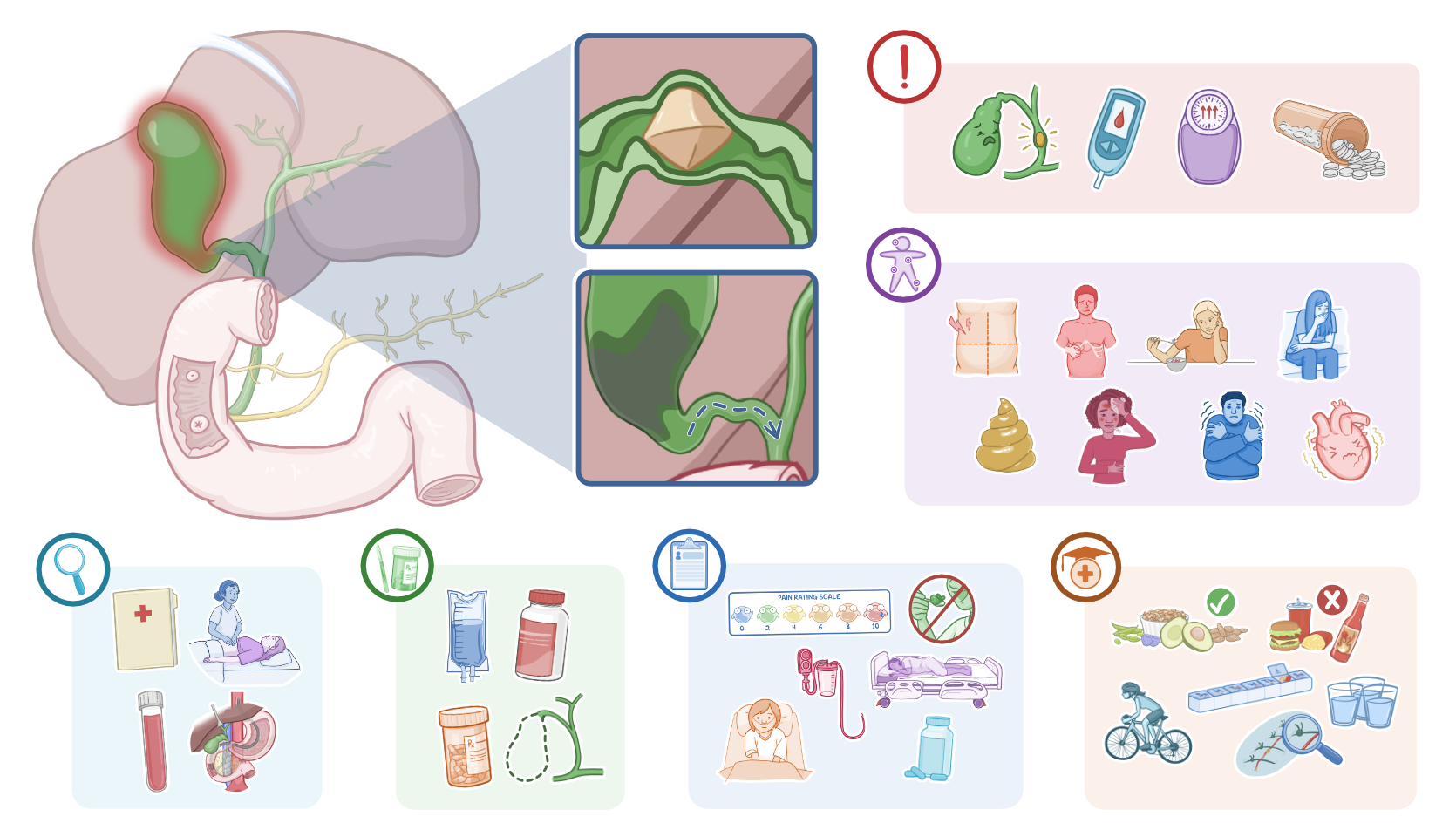
Cholecystitis refers to inflammation of the gallbladder, which is a small, pear-shaped organ located beneath the liver.
Now, let’s quickly review some anatomy and physiology. The biliary tree is made of the liver, gallbladder, and bile ducts. The liver is in charge of producing bile, which is mostly made up of bile salts and acids, cholesterol, phospholipids, proteins, bilirubin and small amounts of various other compounds, like water, electrolytes, and bicarbonate.
Then, bile flows out of the liver through the hepatic ducts towards the gallbladder, where it’s stored. Now, eating fatty foods stimulates the cells in the small intestine to secrete cholecystokinin into the bloodstream. Cholecystokinin, in turn, stimulates the gallbladder contraction, causing it to release bile through the cystic duct and then the common bile duct.
Finally, the common bile duct joins the pancreatic duct, forming the ampulla of Vater, which is surrounded by the sphincter of Oddi. This sphincter acts as a one way valve that allows bile and pancreatic juice to be drained into the duodenum, but prevents backflow from the duodenum into the pancreatic and common bile ducts. Once in the duodenum, bile acts as a fat emulsifier, which essentially helps to digest lipids from food into small micelles, making them easier to absorb.
Now, cholecystitis is caused by biliary stasis, meaning that the bile flow is impaired. Depending on the underlying cause, cholecystitis can be classified as calculous or acalculous. The most common type is calculous cholecystitis, where biliary stasis is caused by cholelithiasis, or a gallstone, obstructing the cystic duct. On the other hand, in acalculous cholecystitis, biliary stasis is caused by gallbladder dysfunction, leading to impaired gallbladder emptying in the absence of gallstones; most often, this occurs due to ischemia of the gallbladder, mainly in hospitalized clients who are critically ill.
Risk factors for cholecystitis include cholelithiasis, diabetes, and obesity; as well as certain medications that decrease gallbladder emptying, like opioids; and conditions that lead to prolonged fasting, dehydration, or immobility, such as having cancer, sepsis, severe trauma or burns, as well as undergoing major abdominal surgery, and receiving parenteral nutrition for an extended period of time.
Now, cholecystitis can be acute or chronic. In acute cholecystitis, bile builds up inside the gallbladder, which causes irritation of the mucosa lining its walls. This also causes pressure in the gallbladder to increase, leading to wall distension and inflammation. If this happens repeatedly, over time, clients may develop chronic cholecystitis, where the ongoing inflammation may cause the gallbladder to undergo fibrosis and calcification. This can ultimately lead to a condition called porcelain gallbladder, in which the gallbladder becomes hard and brittle.
Now, both acute and chronic cholecystitis may lead to serious complications. For starters, once the bile flow is blocked, intestinal bacteria like Escherichia coli or Klebsiella and Enterococcus species, can slowly make their way up the biliary tract and cause infection; this is known as ascending cholangitis.
On the other hand, if the cholecystitis isn’t resolved and the pressure in the gallbladder keeps building up, it may start pushing down on the blood vessels supplying the gallbladder; as a result, the gallbladder starts to get ischemic, leading to gangrenous tissue death, so the wall might eventually perforate, ultimately leading to peritonitis and even sepsis.
Now, symptoms of acute cholecystitis include acute, severe, and prolonged abdominal pain in the right upper quadrant or the epigastric region; in some cases, the pain can be referred to the right shoulder, which is known as Boas sign. In addition, clients typically present with a positive Murphy sign; this is tested by deeply palpating the costal margin at the right upper quadrant, and then asking the client to take a deep breath; so, as the diaphragm pushes down on their inflamed gallbladder, it will cause sharp pain, forcing the client to stop breathing in further.
Other signs and symptoms include anorexia, nausea, vomiting, and intolerance for fatty foods, which may result in steatorrhea or greasy, foul-smelling stools. Finally, some clients may develop jaundice, as well as fever, chills, and tachycardia.
On the other hand, chronic cholecystitis presents with episodes of vague and steady abdominal pain, which may also be referred to the right shoulder; as well as heartburn, nausea and vomiting, intolerance for fatty foods, and some clients may develop jaundice.
Diagnosis of cholecystitis starts with history and physical assessment, followed by laboratory tests showing leukocytosis and with elevated LDH, AST, ALT, and bilirubin blood levels. Diagnosis can be confirmed with ultrasound, which can help detect any gallstones, as well as signs of gallbladder inflammation, such as wall thickening and pericholecystic fluid.
If the diagnosis remains unclear, the site of obstruction can be visualized with other diagnostic tests, including endoscopic retrograde cholangiopancreatography, or ERCP, which can also be used as treatment to remove the gallstone or drain the built up bile; as well as percutaneous transhepatic cholangiography, and hepatobiliary or HIDA scan.
Initial treatment of cholecystitis often includes supportive measures like intravenous fluids, pain management, and antibiotics. The definitive treatment for cholecystitis is cholecystectomy, which is surgical removal of the gallbladder. If surgery can’t be performed, an alternative treatment option is gallbladder drainage, either percutaneously or via ERCP.
Okay, let’s look at the nursing care you’ll provide for a client with cholecystitis. Your priority goals are to monitor for complications; as well as provide supportive care to relieve symptoms like fever, nausea, vomiting, and pain.