Complete metabolic panel (CMP) - Potassium: Nursing
Notes
| POTASSIUM | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
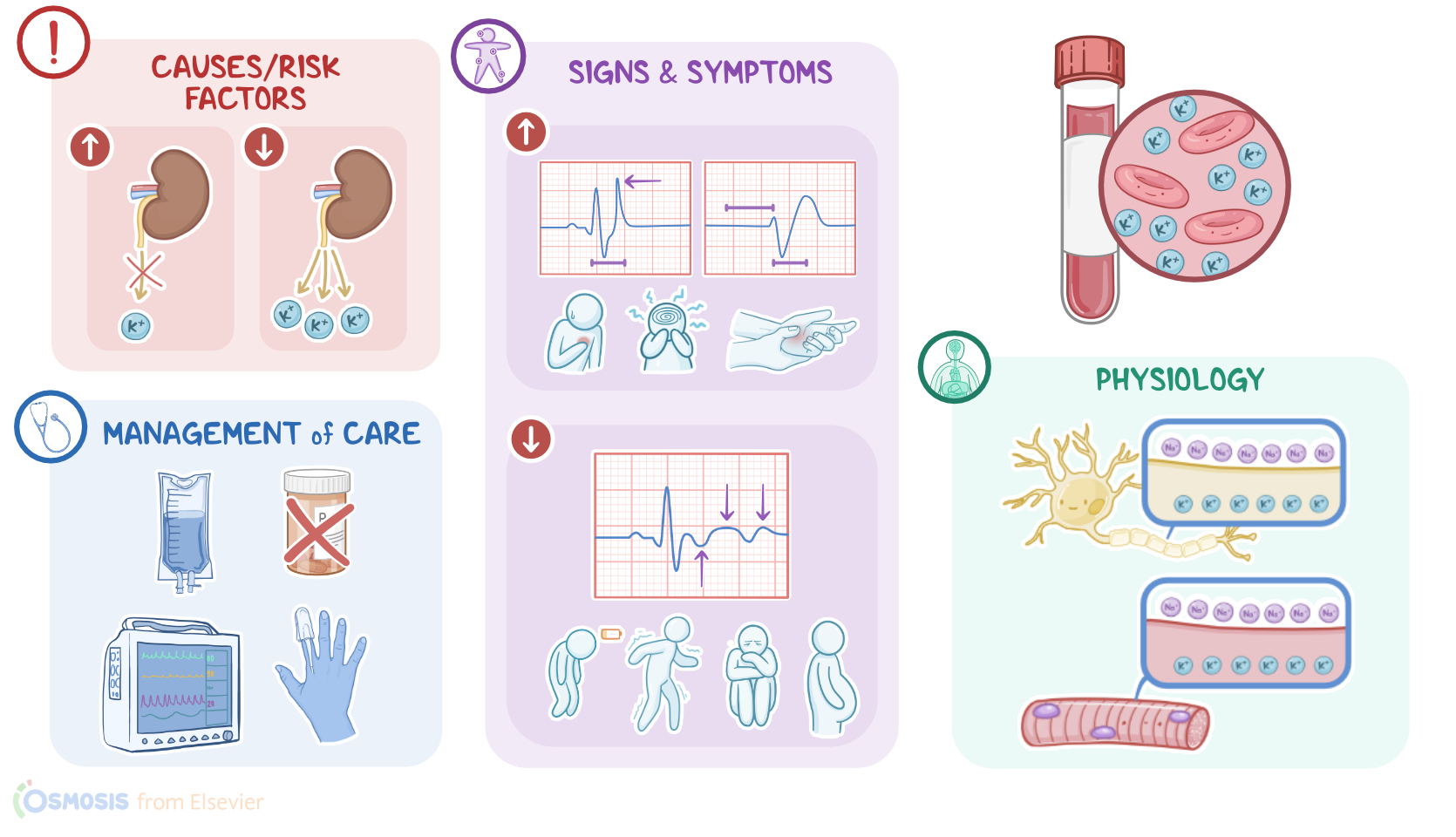
A client with a history of chronic kidney disease arrives at the emergency department via ambulance and reports feeling weak and experiencing palpitations. The electrocardiogram, or ECG, reveals peaked T waves and a prolonged QRS interval. Based on these findings, a complete metabolic panel, or CMP, is ordered to check their serum potassium level. Now, potassium, which has the symbol K+, is a positively charged ion, or cation. About 98 percent of the body’s total potassium is found in the intracellular fluid, while the remaining 2 percent is in the extracellular fluid. Potassium mostly comes from the diet, and once ingested, a tiny amount is excreted through sweat and the gastrointestinal tract, while most of the excess potassium is excreted by the kidneys.
A normal potassium concentration is essential for maintaining the overall electrochemical gradient across the membrane of each cell, which supports nervous system function, and the contraction of skeletal, smooth, and cardiac muscles. So, the plasma level of potassium can be measured on its own or as part of a CMP or a complete metabolic panel; which is also called a basic metabolic panel, or BMP. This level represents the amount of potassium in the plasma. In adults, normal potassium levels range from 3.5 to 5.1 mEq/L. Critical values are 2.5 mEq/L or less and 6.0 mEq/L or more. All right, now there are certain conditions that can alter a client’s potassium level. The three primary causes of a high potassium, or hyperkalemia, are decreased potassium excretion, increased potassium intake, and a potassium shift from inside the cells to outside the cells.
First, let’s look at decreased potassium excretion. This can occur from conditions like acute or chronic renal disease; or the use of certain medications, like potassium-sparing diuretics such as spironolactone; non-steroidal anti-inflammatory drugs, or NSAIDs, like ibuprofen; and angiotensin converting enzyme, or ACE, inhibitors, like captopril. Decreased potassium excretion can also be caused by adrenal cortex dysfunction due to disorders like Addison disease, because dysfunction of the adrenals leads to low levels of aldosterone, which results in increased sodium excretion and excess potassium retention. The next cause of hyperkalemia is from an increased intake of potassium. This can come from taking oral potassium supplements, overuse of salt substitutes, intravenous infusions of potassium, or medications that contain potassium, such as penicillin K.
Lastly, hyperkalemia can occur when potassium shifts out of the cells. This can happen when there’s an acid-base imbalance, like acidosis, which is excess acid in the serum, and a low pH. In acidosis, hydrogen, which is an acid and a positively charged ion, moves into the cell to reduce the acid concentration in the plasma. This will cause potassium to shift out of the cell so that the amount of positive ions in and out of the cell remains constant. Although this helps with acidosis, the levels of potassium in the plasma increase. Another way that potassium escapes the cell is through cellular damage. When cells are damaged it can lead to the release of potassium from the cells into the plasma. This cell damage can come from a crush injury, burn, chemotherapy, or from rhabdomyolysis which is a condition that causes the destruction of skeletal muscle tissue.
Now, if the serum potassium level is too high, clinical manifestations can include heart palpitations, paresthesias, muscle weakness, decreased deep tendon reflexes, and an altered mental status. The client can also experience gastrointestinal symptoms like nausea, diarrhea, and abdominal cramping. Severe hyperkalemia can lead to flaccid paralysis, and difficulty breathing due to impaired respiratory muscles. There can also be ECG changes, like peaked T waves, ST segment depression, short QT interval; and in severe hyperkalemia, there might be absent P waves, a prolonged PR interval, or a wide QRS complex. Ventricular arrhythmias may also occur.
At the other end of the spectrum is hypokalemia, which is when the level of potassium in the serum is too low. Hypokalemia can have several causes, like when too much potassium is lost; when there is an increased production of aldosterone; when too much potassium shifts into the cells, or from inadequate potassium intake. So, the first possible cause of hypokalemia is from an excessive loss of potassium from the gastrointestinal tract from excessive diarrhea and vomiting, or from the kidneys due to the use of diuretics, such as thiazides and loop diuretics. The next cause of hypokalemia is from adrenal tumors or certain genetic conditions that lead to increased production of aldosterone, and ultimately, increased sodium retention and potassium excretion.