Contraception - Natural methods: Nursing
Notes
| CONTRACEPTION - NATURAL METHODS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CALENDAR METHOD |
| |
| STANDARD DAY'S METHOD |
| |
| SYMPTO-THERMAL METHOD |
| |
| LACTATIONAL AMENORRHEA |
| |
| COITUS INTERRUPTUS |
| |
Transcript
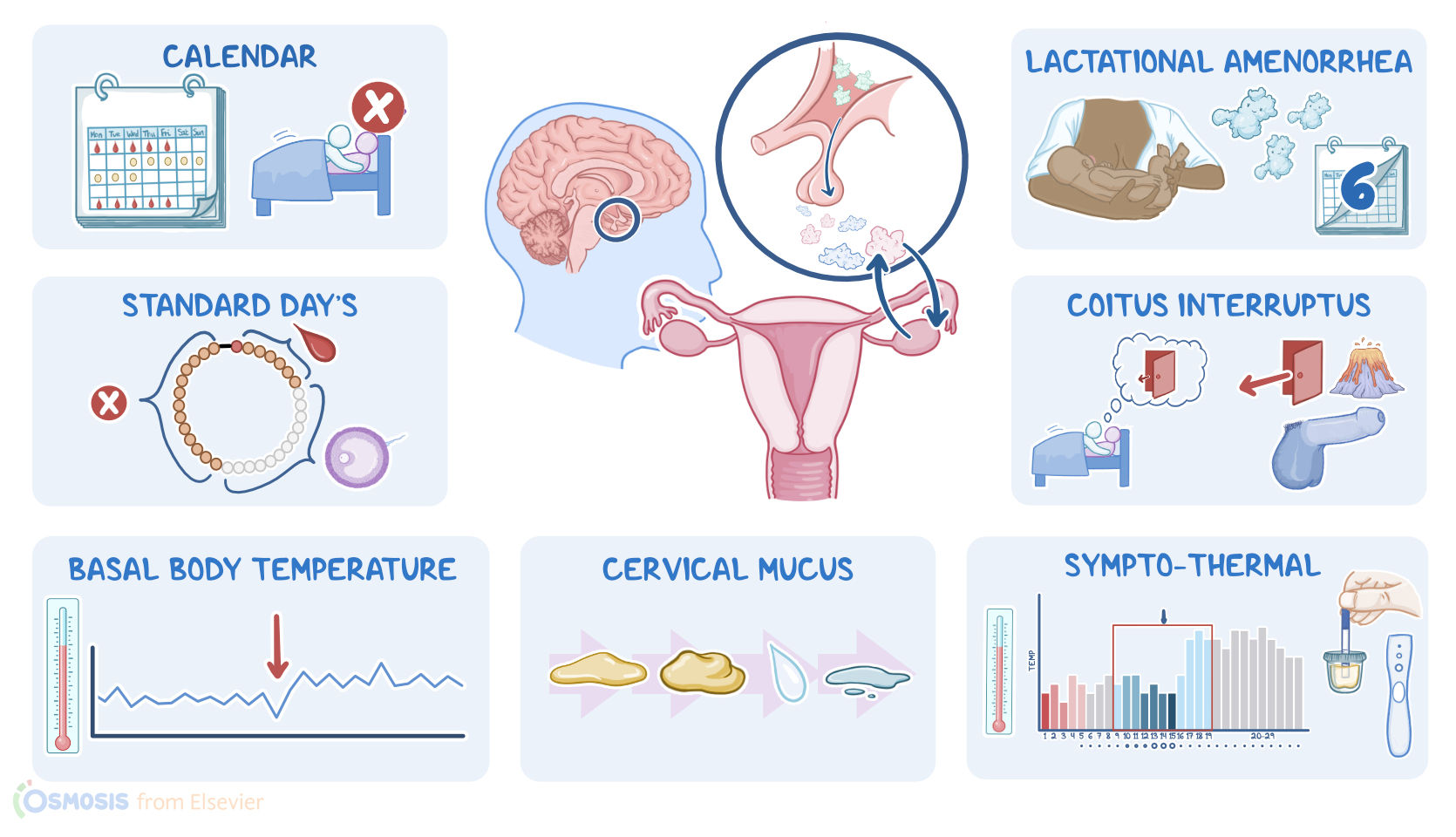
Natural methods of contraception, also referred to as fertility awareness or periodic abstinence methods, are contraception methods that use certain physiologic cues to predict ovulation, and determine the time when fertilization is most likely to occur. Knowing this can be used either to increase the likelihood of becoming pregnant or to avoid it. Natural methods of contraception include the calendar method, standard day’s method, basal body temperature method, the cervical mucus method, the sympto-thermal method, lactational amenorrhea, and finally, coitus interruptus.
All right, now, let’s go over the physiology of the ovaries, which are the gamete and hormone producing organs in clients assigned female at birth. The ovaries contain ovarian follicles, which house the female gametes, called oocytes. Ovarian follicles also secrete the hormones estrogen and progesterone, which have a key role in the menstrual cycle and ovulation. Hormone production, as well as ovulation, which refers to the release of an oocyte each month, is under the control of the hypothalamus and the pituitary gland, way up at the base of the brain.
So, the hypothalamus secretes gonadotropin releasing hormone, or GnRH, which tells the pituitary to secrete follicle-stimulating hormone, or FSH, and luteinizing hormone, or LH. FSH stimulates the maturation of a dominant ovarian follicle each month during the follicular phase of the menstrual cycle, which goes from the first day of menstruation until day 14 of an average 28 day cycle. As the dominant follicle matures, it secretes more and more estrogen, which acts as a negative feedback signal, meaning it tells the pituitary to secrete less FSH and LH. That is how it goes until day 14, which is when ovulation occurs.
Now, right before ovulation, estrogen levels increase past a critical point, and they become a positive feedback signal. This basically tells the pituitary that enough estrogen has been produced for ovulation to occur. In turn, the pituitary secretes a surge of FSH and LH, which causes the ovarian follicle to rupture and release the oocyte in the fallopian tube, where it can be fertilized by a sperm. Estrogen also causes the cervical mucus to increase in amount and become thin, slippery, so that it’s more hospitable to sperm.
After ovulation, comes the luteal phase of the menstrual cycle, which lasts from day 15 to day 28 of an average 28 day cycle. During this phase, the remains of the ovarian follicle become the corpus luteum, which secretes progesterone that thickens the endometrial layer, to get it ready for implantation of a potentially fertilized egg. Progesterone also acts as a negative feedback signal for LH, preventing a second ovulation from occuring in the same month. Progesterone also causes the cervical mucus to dry up. At the same time, the progesterone surge may lead to a slight increase in the basal body temperature, compared to the first half of the menstrual cycle.
Now, if fertilization doesn’t occur, the corpus luteum degenerates, and progesterone levels decrease. At this time, the cervical mucus becomes thicker to prevent the entrance of sperm, but also decreases, and becomes less noticeable. Low progesterone also causes the innermost layer of the uterus, called the endometrium, to slough off, which starts menstruation and a brand new menstrual cycle. Now, a factor that can affect the menstrual cycle is breastfeeding. That’s because suckling and breastfeeding increases the secretion of prolactin, which in turn inhibits the hypothalamic-pituitary-ovarian axis that controls ovulation and menstruation, so typically, during breastfeeding the mother can not get pregnant again.
With that in mind, let’s go through the various natural methods of family planning, starting with the calendar method. This is based on tracking the length of at least 6 cycles and expecting ovulation at approximately 14 days before the onset of menses. So, to predict the approximate first fertile day of a menstrual cycle, the client should find the shortest cycle in their record and subtract 18 from the total number of days in that cycle. Likewise, for the last fertile day, the client can subtract 11 days from the total number of days in the shortest cycle of their record. In order to avoid conception, the client should either abstain from intercorse or use another form of contraception throughout the fertile period.