Delirium: Nursing
Delirium: Nursing
Watch later
Watch later
Notes
| DELIRIUM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Delirium is a sudden, waxing and waning decline in various mental functions, including memory, thinking, language, behavior, mood, and personality.
Let’s start by looking at the anatomy and physiology of the brain, which has three main parts, called the cerebrum, which consists of the two cerebral hemispheres, the cerebellum, which sits down at the base of the skull, and the brainstem, which is located right in front of the cerebellum.
Zooming in, the cells that make up our brain are called neurons. Neurons are composed of a cell body, which contains all the cell’s organelles, and nerve fibers that extend out from the neuron cell body. These nerve fibers are either dendrites that receive signals from other neurons or axons that send signals along to other neurons.
Neurons communicate with each other through neurotransmitters, such as acetylcholine, dopamine, norepinephrine, and glutamate.
Now, the brain is responsible for various mental functions, including memory, language, personality, visuospatial function, concentration, executive function, and praxis, which is the ability to carry out complex motor activities.
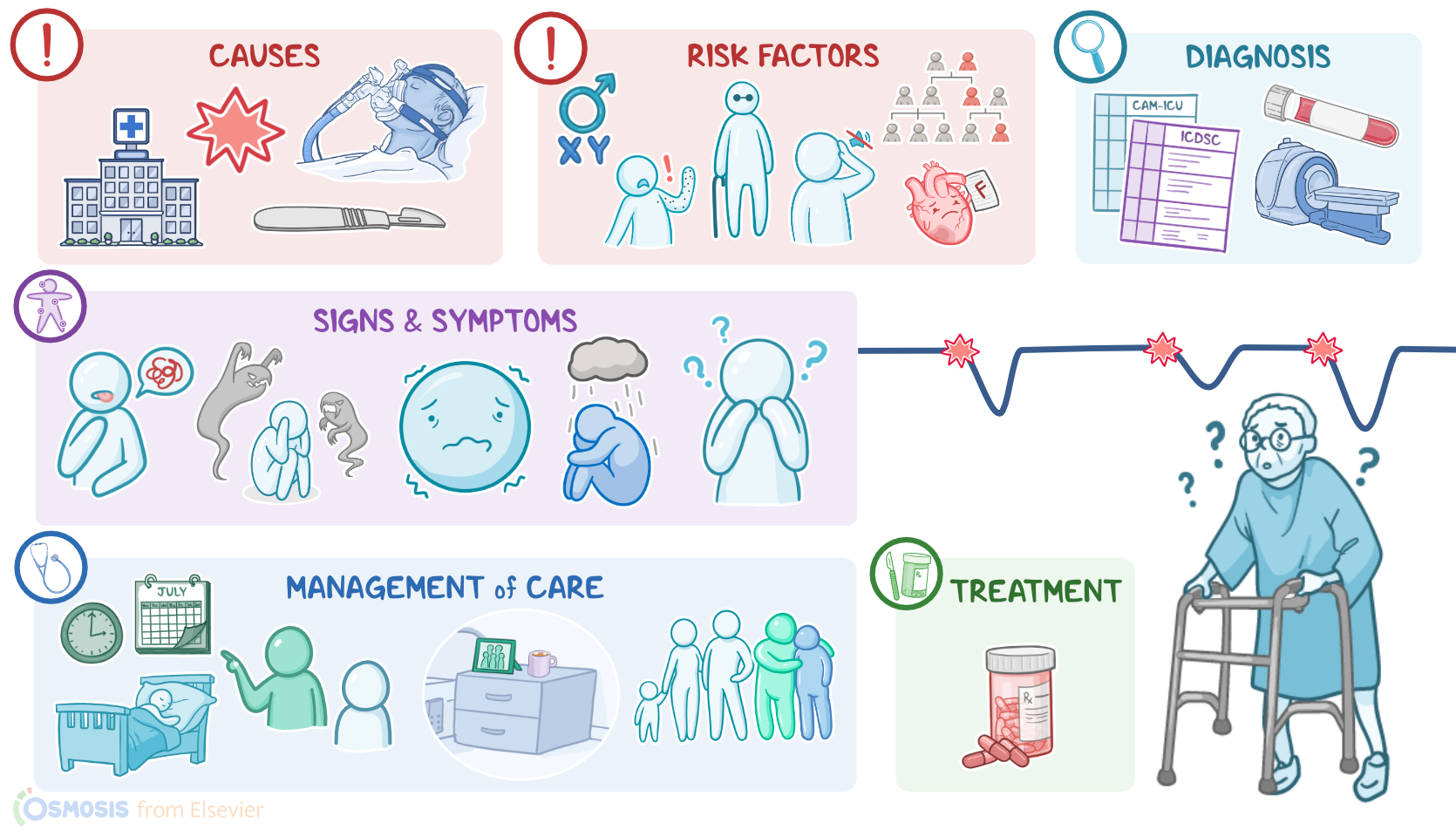
Okay, now, delirium usually occurs as a consequence of an underlying condition, which can include infections, medication toxicity, particularly with the use of sleep medications or aminoglycosides, and electrolyte imbalances.
Other causes include severe stress, pain, sleep deprivation, dehydration, or malnutrition. Delirium can also occur after a recent hospitalization, surgery, or use of mechanical ventilation, as well as after trauma.
Now, risk factors for developing delirium include advanced age; being assigned male at birth, and personal or family history of delirium. Clients with dementia or psychiatric disorders, such as depression and schizophrenia, are also more likely to develop delirium. Finally, delirium is more common in clients with underlying medical conditions, such as heart failure, cancer, and diabetes, as well as in those with visual or hearing impairment.
So, pathology-wise, the exact mechanism that leads to delirium is not clear. One theory is that the oxidative metabolism of the brain gets impaired, leading to low oxygen levels in the brain. Another theory is that delirium is caused by abnormal levels of neurotransmitters in the brain.
It is also thought that in delirium, neuronal membranes may not be able to depolarize properly, and therefore, the action potential cannot be transmitted from one neuron to another.
Alternatively, delirium might have to do with inflammatory cytokines that get released during infection or trauma and interfere with neuronal function.
Okay, moving on to clinical manifestations. Delirium typically has a sudden onset and can last hours or weeks. Signs and symptoms can come and go. You might notice your client isn’t their usual self, which could signal the onset of delirium.
Other common behaviors include disorientation, meaning they don't know where they are or what day it is; or they might have difficulty concentrating.
Based on the level of activity, delirium can be classified as hypoactive, hyperactive, or mixed, where their activity fluctuates. The client’s emotional state can also range from being agitated, angry, and aggressive to drowsy, withdrawn, and depressed.
Their speech may not make sense; they could experience hallucinations, which means they see, hear, or even smell things that are not actually real but are very real to them; or they could experience delusions, where they believe things that are not true.
Now, clients with delirium can be more prone to complications. When clients are feeling disoriented, agitated, and confused, they can easily stumble and fall. These falls can lead to painful consequences including bone fractures, and head injuries, as well as bruises and bleeds.
In general, clients with delirium often end up having prolonged hospitalizations, more medical complications of the underlying conditions, and ultimately higher mortality rates.
Alright, now the diagnosis of delirium is typically based on the client’s history and physical assessment. Most of the time, a close family member, a friend, or a healthcare provider notices the client’s sudden change in behavior and cognition.
To confirm the diagnosis, dementia and sundown syndrome must be excluded. So, in contrast to delirium, dementia has a gradual onset, lasts months to years, and progressively worsens over time.
Sundown syndrome occurs in clients with dementia in which symptoms of confusion or loss of orientation intensify when the sun goes down, meaning in the afternoon or evening.
In addition, certain screening tools like Confusion Assessment Method for the ICU, or CAM-ICU, as well as the Intensive Care Delirium Screening Checklist, or ICDSC can be used to assess the client.
Now, after the diagnosis of delirium is confirmed, the specific cause can be identified based on lab tests and appropriate imaging tests, including X-rays and scans.
Moving on to treatment, delirium is a medical emergency that must be recognized and treated promptly. The good news though is that delirium is often reversible when the underlying condition is resolved. In addition, low doses of antipsychotic medications like haloperidol can be administered as needed.