Ectopic pregnancy: Nursing
Notes
| ECTOPIC PREGNANCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
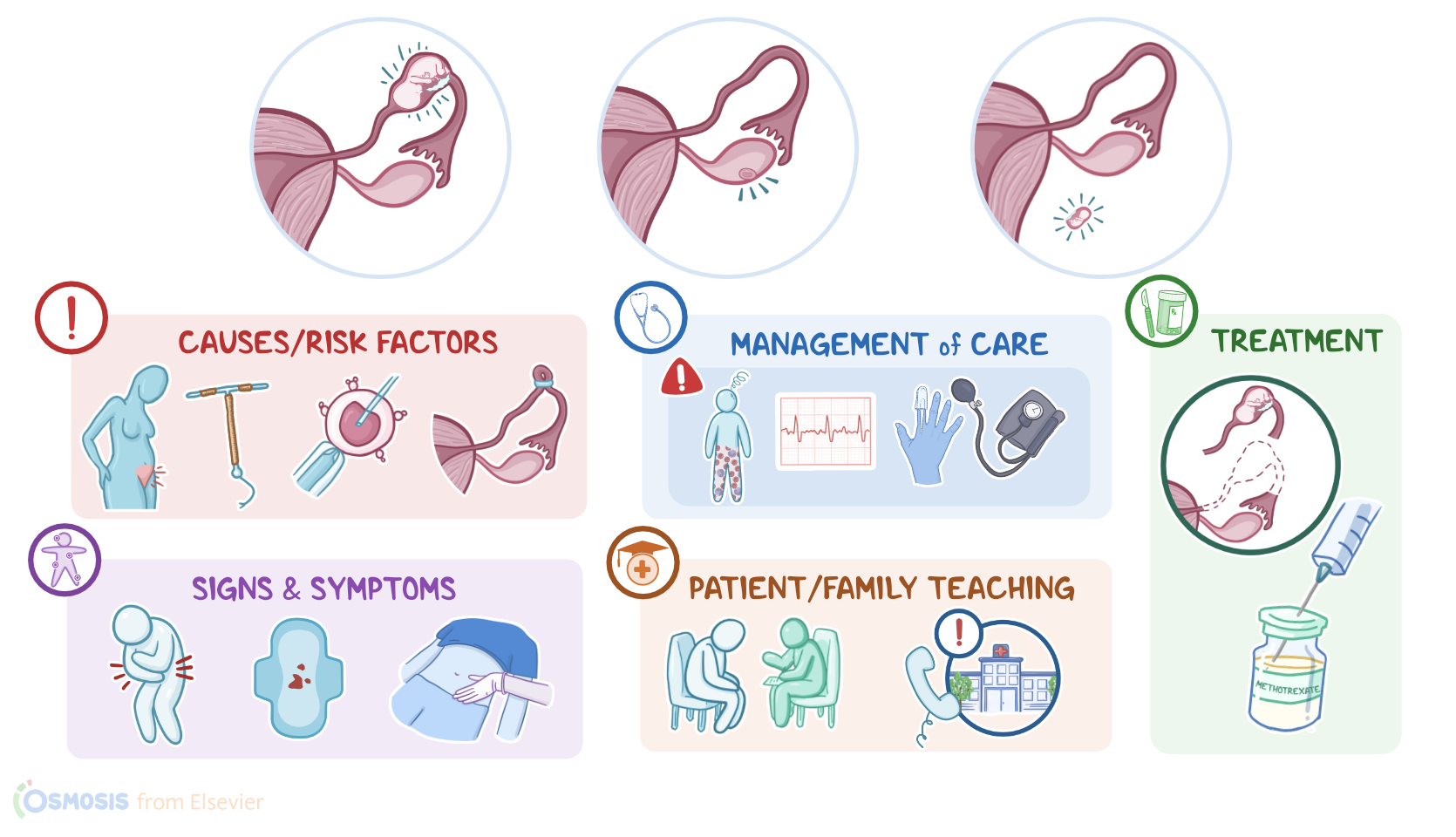
An ectopic pregnancy is a pregnancy that occurs somewhere other than in the uterine cavity, most commonly in one of the fallopian tubes.
Alright, now let’s quickly review the physiology of fertilization, starting with the ovaries, which are the paired female gonads. Each month, they release one mature egg, also called oocyte, which is the female gamete. After leaving the ovaries, this egg enters the fallopian tube and reaches the widest part of it, called the ampulla of the fallopian tube. This is where the few sperm that have made it this far after ejaculation surround the egg; and of them, a single sperm succeeds in entering the egg and fertilizing it, forming the zygote. The zygote then makes its way through the fallopian tube in order to reach the uterus; where it implants in the endometrium, also called the uterine lining. At the same time, the endometrial tissues react to a surge in progesterone released from the ovaries, and engorges with blood and fluids, to become a cozy home for the future embryo.
Now, the cause of an ectopic pregnancy in any given client is often unknown, but there are several risk factors. These include cigarette smoking; a history of pelvic inflammatory disease; conception by in-vitro fertilization; gynecologic surgery; current use of intrauterine devices; tubal ligation; or a previous ectopic pregnancy. All of these factors contribute to the formation of scar tissue within the fallopian tube, which in turn prevents the progress of the embryo into the uterus, causing it to attach to the tube itself.
Now, pathology-wise, in the vast majority of ectopic pregnancies, the embryo does not complete its journey to the uterus and implants in the fallopian tube, and this is called a tubal pregnancy. However, there are also ovarian ectopic pregnancies, in which case, the egg never leaves the ovary; as well as abdominal ectopic pregnancies, when the egg is “lost” to the abdominal cavity following ovulation, instead of entering the fallopian tube.
After ectopic implantation, the embryo begins developing and growing. Over time, the tissue can no longer provide enough blood supply for the embryo, causing a spontaneous abortion. On the other hand, if the tissue can supply the embryo with enough blood, then hormones released by the ovaries and placenta can cause early pregnancy signs like a missed menstrual period and other body changes, like nausea and fullness of breasts.
When the ectopic pregnancy occurs in the fallopian tube, the growing embryo eventually runs out of space and damages the walls of the tube, potentially causing the tube to rupture. A ruptured ectopic pregnancy is a medical emergency, as it can cause massive hemorrhage into the abdominal cavity and hemodynamic instability.
Clinically, besides the early signs of pregnancy, signs of an ectopic pregnancy can include abdominal or pelvic pain and vaginal bleeding, possibly accompanied by a palpable mass near the uterus. Typically, these symptoms appear around 6 to 8 weeks into the pregnancy, but if the ectopic pregnancy occurs in a place with a lot of space for the embryo to grow, pain and bleeding may not occur until several weeks later. In cases complicated by a ruptured tube, there could be severe, acute abdominal or pelvic pain, and referred pain to the shoulder due to blood irritating nerves in the diaphragm. There can also be signs of hemodynamic instability, such as pallor, tachycardia, or hypotension.
The diagnosis of an ectopic pregnancy starts with the client’s history and physical assessment. The next step is to confirm the pregnancy with a β-hCG test and to perform a transvaginal ultrasound to see whether or not there’s an intrauterine pregnancy. The transvaginal ultrasound can also help identify an ectopic pregnancy based on signs like excess fluid in the peritoneal cavity or the presence of a mass in the fallopian tube. Now, when it comes to treatment, it’s worth noting that uncomplicated ectopic pregnancies often resolve spontaneously. In the remaining cases, treatment may involve close monitoring, medications, or surgical intervention. In clients whose ectopic pregnancy is diagnosed early and the β-hCG is already declining, treatment includes close monitoring and serial β-hCG measurements, with no additional medications or procedures. If the ectopic pregnancy is identified later, then methotrexate can be used to terminate the pregnancy. Finally, if there are signs of a ruptured tube, a salpingostomy can be done. That’s where the fallopian tube is opened up to remove the pregnancy, and then closed at the end of surgery. Alternatively, a salpingectomy can be done, which is where the fallopian tube is completely removed. Finally, if the mother is Rh negative, it’s important to give her RhoD immunoglobulin. This is because if the fetus is Rh positive, exposure to fetal blood could cause the mother’s immune system to make anti-Rh antibodies. These antibodies can harm an Rh positive fetus in future pregnancies, because they can bind to fetal RBCs in the Rh positive fetus, leading to hemolysis.
Alright, let’s discuss the nursing care for a client with an ectopic pregnancy. Your priority goals of care include early recognition and management of tubal rupture, hemorrhage, and hypovolemic shock; and providing emotional support.