Flail chest: Nursing
Flail chest: Nursing
Acute Final
Acute Final
Notes
| FLAIL CHEST | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
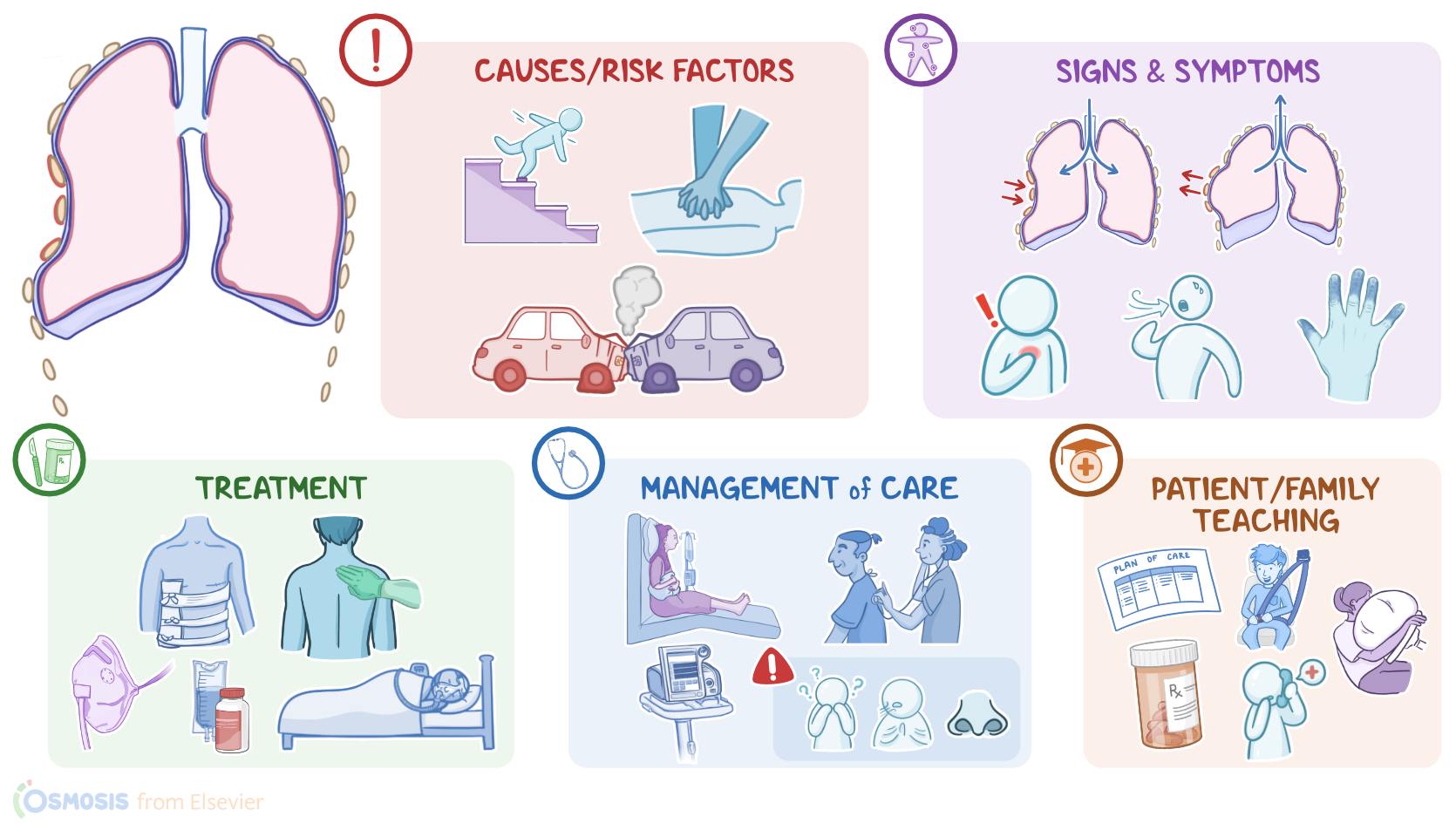
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Flail chest is a serious condition, often caused by severe blunt chest trauma. It occurs when multiple consecutive ribs are fractured, creating a separate, free floating section of ribs and connecting tissue that moves out of sync with the rest of the chest during breathing.
First, let’s quickly look at the anatomy and physiology of the thoracic cage. The thoracic cage is made up of 12 pairs of ribs and the sternum, which together create the shape of the chest wall and protect thoracic structures, such as the heart, lungs, and blood vessels.
Now, the key muscles involved in breathing are the intercostal muscles, which are located between each set of ribs, and the diaphragm, which covers the whole bottom of the thoracic cage. When a person inhales the diaphragm contracts, moving downward and the intercostal muscles contract to move the rib cage out. This increases the volume while decreasing pressure in the thoracic cavity. The change in pressure pulls air down into the lungs. In contrast, when a person exhales the diaphragm and intercostal muscles relax which decreases the volume, while increasing pressure in the thoracic cavity. This makes air move out of the lungs.
Now, the main cause of a flail chest is blunt trauma to the chest, which can be caused by falls, abuse, car crashes, crush injuries, or even cardiopulmonary resuscitation.
Risk factors for a flail chest include modifiable ones, such as intoxication, and practicing contact sports; as well as non-modifiable ones, such as advanced age, and being assigned male sex at birth.
Okay, now, the pathology of a flail chest begins when a blunt trauma causes three or more ribs to fracture in two or more places, or when there’s bilateral detachment of ribs from the sternum. This creates a segment of the ribs that is not mechanically attached to the rest of the chest wall, As a result of these two pathologies, the chest moves in a paradoxical or uncoordinated fashion. This means that when the person breathes in, the chest wall expands, pulling outwards, but intrathoracic pressure becomes more negative, pulling the unattached segment inwards. On the other hand, when the person breathes out, the chest wall contracts, pulling inwards, but intrathoracic pressure becomes more positive, which pushes the separated section outwards.
Damage to the thoracic wall also prevents the lungs from expanding fully which impairs respiration. In addition,the intercostal muscles pull on the broken rib segment during breathing which causes severe pain and further impairs breathing.
Now, flail chest is also associated with several complications, the most common of which is pulmonary contusion, or injury of the lung parenchyma. This can cause atelectasis or collapse of the alveoli in the lung. These collapsed alveoli can’t participate in gas exchange, causing shunting, so blood doesn't become oxygenated as it moves through the lungs.
This can result in acute, refractory hypoxemia, meaning that the client’s oxygenation does not improve even when they receive higher concentrations of oxygen; and ultimately, clients develop acute respiratory distress syndrome, or ARDS. Since clients with flail chest have trouble breathing or coughing up airway secretions, they are also at an increased risk of developing pneumonia. Another complication is pneumothorax, which is when there’s air in the pleural cavity, and that doesn’t allow the lung on that side to expand properly. Finally, in severe cases, the broken ribs can tear the aorta, damage the diaphragm, or injure internal organs like the spleen, liver, or kidneys.
Typically, the clinical manifestations of flail chest include paradoxical breathing, along with pain at the sites of the fractures, which intensifies with breathing, moving, coughing, or even sneezing. Some clients also splint, meaning that they take short, shallow, rapid breaths in an effort to limit chest movement and reduce pain. In severe cases, they may also experience shortness of breath, cyanosis, and refractory hypoxemia. Additionally, clients can develop hemodynamic instability, which presents as hypotension, tachycardia, or arrhythmias.
During auscultation of the chest, there are diminished breath sounds, and palpation of the chest typically reveals crepitus, which refers to crunching or grinding sounds, when the site of the fracture is moved.