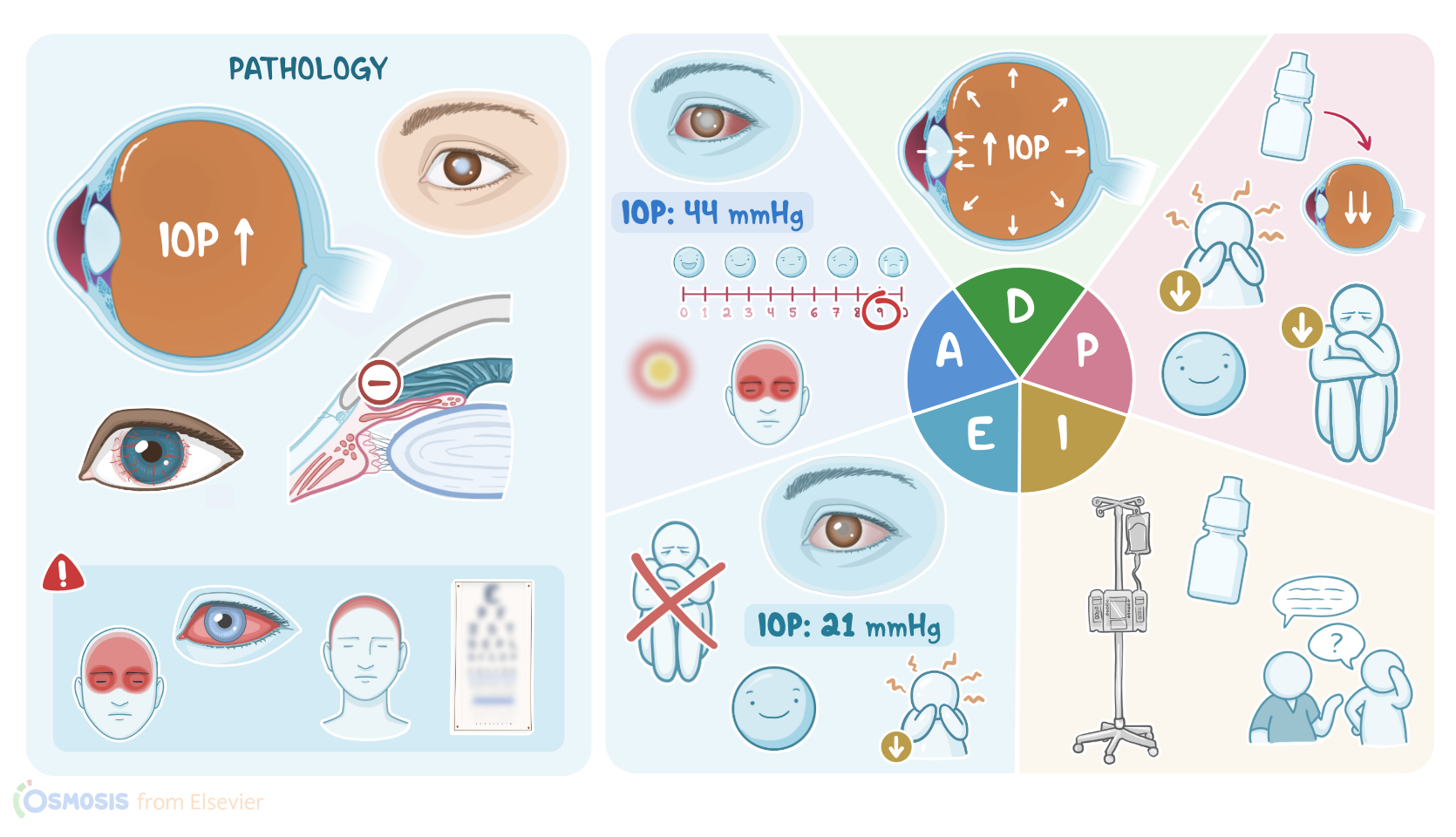
Glaucoma: Nursing process (ADPIE)
Glaucoma: Nursing process (ADPIE)
SHRAVAM
SHRAVAM
Notes
| GLAUCOMA | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Mrs. Barbara Yao is a 67-year-old female client who was brought by her husband to the emergency department, or ED, with reports of blurred vision, eye pain, a severe headache, and nausea for the past two hours. She states that she sees red halos around lights and you notice her eyes appear red. The ED physician diagnoses her with acute angle-closure glaucoma.
Glaucoma refers to a group of eye conditions that are associated with increased pressure in the eye, referred to as intraocular pressure, or IOP. But, before we proceed with glaucoma, first, let’s take a look at a cross-section of the eye. On one side of the lens, we have anterior and posterior chambers filled with the fluid aqueous humor; while on the other side, we have the vitreous body filled with the gel-like vitreous humor. Now, the aqueous humor is secreted by the ciliary epithelium into the posterior chamber, and from here, it flows through the pupil to the anterior chamber. Next, from the anterior chamber, the fluid drains out of the eye through the trabecular meshwork, into the Sclemm’s canal, and eventually into the aqueous veins. Controlled production and drainage result in normal intraocular pressure, which typically ranges from 10 to 20mmHg.
Now, in glaucoma, drainage of aqueous humor is restricted. As a result, the aqueous humour builds up and pushes against the vitreous body. This causes intraocular pressure to rise which eventually leads to damage to the optic nerve and the retina. Depending on whether or not the angle between the iris and the cornea is obstructed, glaucoma can be defined as open- or closed-angle.
In open-angle glaucoma, which is also known as wide-angle glaucoma, the angle between the cornea and the iris is not obstructed but the trabecular meshwork is. This is the most common type of glaucoma and Black individuals, those with advanced age, or a family history are at a higher risk. Now, open-angle glaucoma can be primary, where the cause is unknown, or secondary to another condition that causes decreased drainage of aqueous humor. These causes include a build up of white blood cells such as in the case of intraocular inflammation; red blood cells, in the case of intraocular bleeding; or even parts of the retina in the case of retinal detachment. Whatever the cause, all clients present with a gradual increase in intraocular pressure. Initially, increased intraocular pressure affects the optic nerve to some extent, decreasing only the client’s peripheral vision at first. But chronic elevated intraocular pressure will result in further damage to the optic nerve and surrounding tissue, eventually causing loss of central vision as well. So, the final stage of injury is the complete, irreversible blindness.
On the flip side, in closed-angle glaucoma, which is also known as angle-closure glaucoma, the angle between the cornea and the iris is obstructed so the aqueous humor can’t reach the trabecular meshwork. Again, closed-angle glaucoma can be primary or secondary. In primary cases, the reason is unknown; whereas the secondary cases are typically caused by conditions that affect the retina and decrease oxygen supply to the eye, like diabetes mellitus or central retinal vein occlusion. This lack of oxygen triggers the process called neovascularization, or the formation of new blood vessels. Some of these new blood vessels can grow into the iris and push it forward, subsequently closing the angle and blocking the outflow. Another secondary cause of closed-angle glaucoma are medications called muscarinic blockers, such as atropine. These medications cause mydriasis, or pupil dilation, thus pushing the iris into the angle and reducing the outflow.
Now closed-angle glaucoma can be acute, in which case the blockage causes a rapid and sharp increase in intraocular pressure, and this is an ophthalmologic emergency. These clients typically present with an abrupt onset of severe pain in the affected eye; ciliary flush, or eye redness; headaches; and vomiting. Additionally, they complain of blurry vision and sometimes see colored halos when looking at a light source. On the other hand, in chronic closed-angle glaucoma, the closure develops gradually so the pressure increases slower so it’s less severe. But, over time, it can also cause damage to the optic nerve and result in blindness if left untreated. Next, individuals with chronic glaucoma have a higher risk of developing long-term complications, such as optic atrophy and cataract formation, or clouding of the lens. Finally, chronic closed-angle glaucoma can cause atrophy of muscles that control the diameter of the pupil, leading to permanent dilation.
Important risk factors that can increase the risk of closed-angle glaucoma include anatomic predispositions, positive family history of glaucoma, older age, and female sex. Also, glaucoma is more common in Asian and Inuit populations. Finally, individuals who have far-sightedness have a higher risk of developing glaucoma because their angle between the cornea and iris is smaller.
Now, the examination of clients with glaucoma typically reveals mid-dilated nonreactive pupils and firm globes, which are often associated with painful eye movements. The diagnosis proceeds with a fundoscopic examination which usually reveals a shallow anterior chamber and a narrow angle between cornea and iris. Additionally, it can reveal “cupping” of the optic disk, which occurs when the tissue around the optic nerve dies, leaving behind an empty space resembling a cup. Next, tonometry can be performed to measure intraocular pressure; while gonioscopy can be performed to evaluate the internal drainage system of the eye, and visual acuity tests can be used to assess and compare visual acuity in each eye. Finally, visual field testing can be ordered to assess the client's peripheral and central vision.
Treatment focuses on medications that decrease the intraocular pressure. This can be done in several ways. First, we can decrease the production of aqueous humor with medications such as beta-adrenergic receptors antagonists, like timolol; and carbonic anhydrase inhibitors, like acetazolamide. Next, we can increase the outflow of aqueous humor with prostaglandin analogs, such as latanoprost. Finally, we can decrease production and increase outflow with medications called alpha-adrenergic agonists, such as epinephrine. Clients who are unresponsive to medications, are candidates for laser interventions.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Inflammation in Glaucoma: From the back to the front of the eye, and beyond" Prog Retin Eye Res (2021)
- "Glaucoma" Med Clin North Am (2021)
- "Advanced glaucoma at diagnosis: current perspectives" Eye (Lond) (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "The Diagnosis and Treatment of Glaucoma" Dtsch Arztebl Int (2020)
- "Glaucoma in Adults-Screening, Diagnosis, and Management: A Review" JAMA (2021)