Group B streptococcus (GBS) infection in pregnancy: Nursing
Notes
| GROUP B STREPTOCOCCUS (GBS) INFECTION IN PREGNANCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Group B streptococcus or GBS for short, is a common bacterium called Streptococcus agalactiae. It is a Gram positive, facultative anaerobe bacteria, meaning it can survive in both aerobic and anaerobic environments. This makes it suited to colonize the gastrointestinal and genitourinary tract; and in healthy, immunocompetent adults, it typically doesn't cause any symptoms. However, in fetuses and newborns, it can cause infections that can lead to major and sometimes fatal complications.
Now, the main cause of GBS infection in pregnancy is when the bacteria colonizes the mother’s genitourinary tract and then gets passed on to the fetus during pregnancy or labor. Common risk factors associated with GBS infection in pregnancy include previous pregnancy with GBS infection, obesity, or Black ethnicity. Finally, preterm delivery, rupture of membranes of more than 18 hours, and vaginal delivery, also increase the risk of newborn GBS infection.
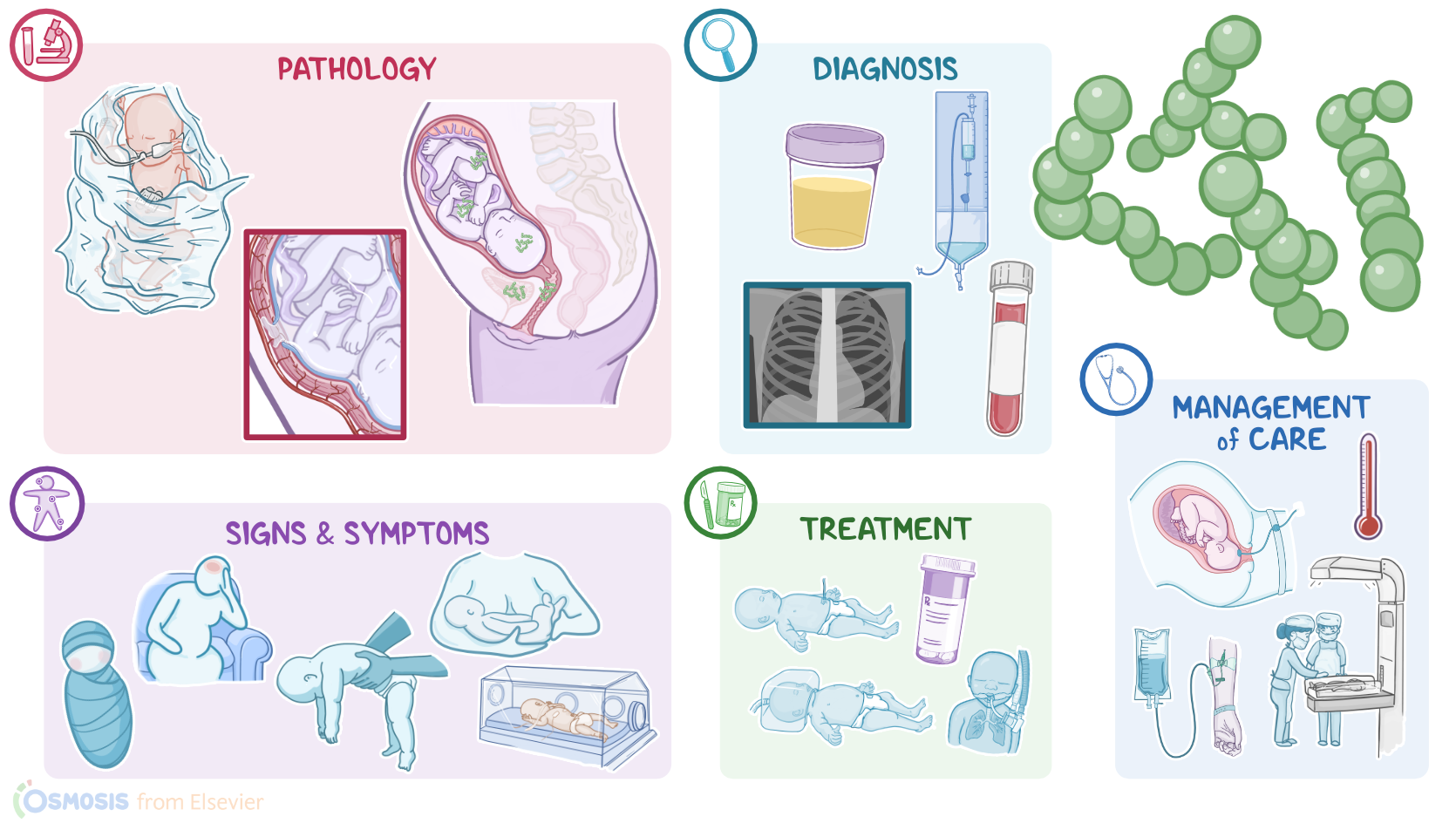
Now, pathology-wise, when GBS colonizes the genitourinary tract, it can ascend into the uterus and infect the fetal membranes, namely the chorion and amnion, causing chorioamnionitis. With chorioamnionitis, the infection can spread to the fetus, causing fetal distress or even intrauterine death. Another consequence is premature rupture of membranes and premature delivery.
On the other hand, GBS can get passed on to the infant during labor when the bacteria is aspirated into the fetal airways. This can cause pneumonia or neonatal sepsis. Alternatively, bacteria from the blood can cross the blood-brain barrier and migrate into the cerebral spinal fluid, causing neonatal meningitis. Meningitis can lead to neurologic sequelae like sight or hearing loss and cerebral palsy. Unfortunately, all three of these conditions can lead to death in some newborns.
Clinically, GBS infections during pregnancy are often asymptomatic. However, an intrauterine infection can cause non-specific symptoms like fever and bacteriuria, and signs of fetal distress like fetal tachycardia. In newborns, on the other hand, there can be signs of early-onset sepsis , when signs develop within seven days after birth; or late-onset sepsis, if they develop between 7 days and three months old. Manifestations can include respiratory distress, temperature instability, difficulty feeding, weak muscle tone, jitteriness, or lethargy.
Diagnosis of GBS infections in pregnancy starts with the pregnant individual’s history and physical assessment. Typically, screening for GBS is done by obtaining cultures from vaginal and rectal swabs at 36 weeks of gestation. If neonatal GBS infection is suspected, blood or spinal fluid cultures can be sent for testing. Other tests that can be performed include urine cultures and chest x-rays, depending on the newborn’s presentation.
Now, regarding treatment, pregnant individuals who test positive for GBS are typically treated with antibiotics during labor. Other indications for antibiotics include if the GBS status is unknown when labor starts, if their membranes have been ruptured for 18 hours or more, if they present with preterm labor, or if they have a fever of at least 100.4 F or 38 C. If newborn infection is suspected or confirmed, treatment includes antibiotics, IV fluids, oxygen, and ventilator support.