Hemolytic uremic syndrome: Nursing
Hemolytic uremic syndrome: Nursing
hematology
hematology
Notes
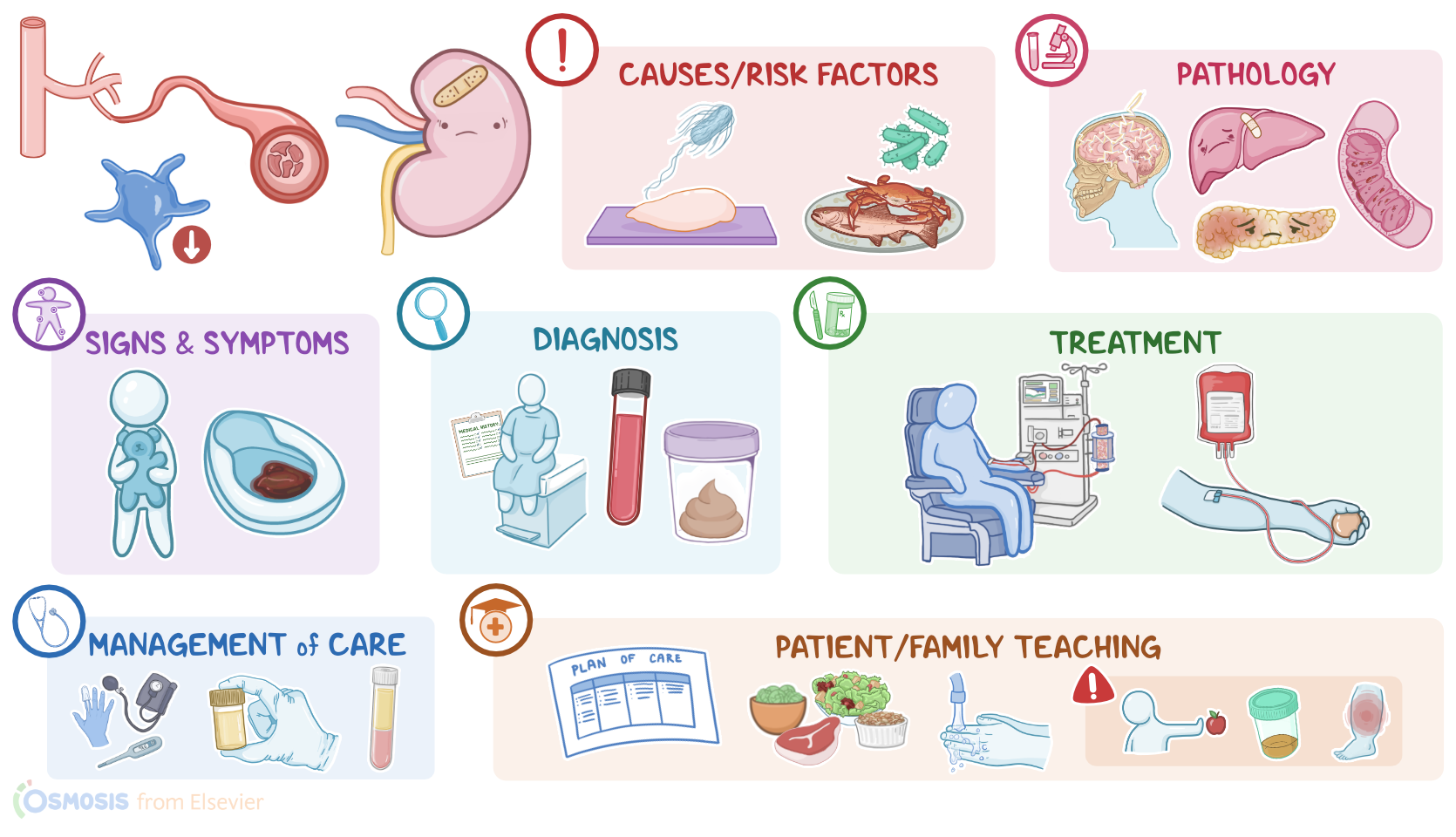
| HEMOLYTIC UREMIC SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Hemolytic uremic syndrome, or HUS for short, is a condition characterized by the triad of microangiopathic hemolytic anemia, or breakdown of red blood cells inside small blood vessels, thrombocytopenia, or low platelets, and acute kidney injury.
Alright, now first, let’s quickly review the physiology behind hemostasis or clotting. Hemostasis starts as a response to an injury of the endothelium, which is the inner lining of blood vessels, and it can be divided into primary and secondary hemostasis. In primary hemostasis, platelets form a “plug” at the site of the damaged blood vessel to stop the bleeding. In secondary hemostasis, proteins called coagulation factors start to activate each other eventually leading to formation of a fibrin mesh around the platelet plug to stabilize it.
Now, the causes of HUS vary, so it can be classified as typical or atypical. Typical HUS is caused by bacterial toxins, including Shiga-like toxin which is produced by some strains of Escherichia coli, most commonly enterohemorrhagic E. coli or EHEC, serotype O157:H7, and Shiga toxin which is secreted by Shigella dysenteriae. These bacteria typically affect children, who become infected through contaminated food or drink, like contaminated beef, raw leafy vegetables, or unpasteurized milk from an infected cow; or by swimming in pools or lakes contaminated with feces. Rarely, typical HUS may also be caused by other bacteria, such as Streptococcus pneumoniae.
On the other hand, atypical HUS is typically non-infectious. It is caused by dysregulation of the complement system, which is part of the immune system, and can be genetic or acquired. The main risk factors for atypical HUS are being above 65 years of age, or having a weakened immune system.
Okay, now, pathology-wise, typical HUS begins when the bacteria enters the body and attaches itself to the intestinal wall and starts secreting toxins. These toxins get absorbed by the intestinal blood vessels and enter the bloodstream.
Once there, they attach to immune cells, or white blood cells, which carry the toxin to the glomerular capillaries in the kidney. Now, the endothelial cells lining these capillaries express a receptor that has an incredibly strong affinity for these bacterial toxins. Basically, this receptor is like a magnet that can simply snatch the toxin away from a white blood cell as it drifts by. Once the toxin binds to the receptor, it gets engulfed by the endothelial cell. Inside the cell, the toxin initiates a number of reactions that eventually result in apoptosis, or cell suicide. And when a large number of endothelial cells undergo apoptosis, hemostasis is triggered; so lots of tiny blood clots form in the kidneys.
This process uses up platelets, causing thrombocytopenia, so there are fewer platelets available in other parts of the body, which can lead to bleeding. At the same time, the presence of blood clots within the narrow capillaries blocks the path for red blood cells, or RBCs, and as they run into the clot, they get damaged and break down, a process called hemolysis, and eventually this can progress to anemia. With more and more clot formation, the renal capillaries get blocked, which leads to acute kidney injury. As a result, the kidneys can no longer dispose of wastes like urea, so it builds up in the blood, causing uremia.
Okay now, HUS can also lead to microthrombi formation and complications in other organs as well. For instance, the central nervous system may be affected resulting in seizures and stroke. Any part of the digestive tract from the esophagus to the anus may be involved, which can cause bleeding; colitis, or bowel inflammation; as well as bowel necrosis and perforations. The liver or pancreas are also frequently affected, causing increased serum transaminases and impaired glucose tolerance, respectively. Long-term complications include chronic kidney disease, or CKD, and hypertension.
Now, clinically, typical HUS most commonly occurs in children, following an episode of bloody diarrhea, so it’s also called diarrhea positive, or D+ HUS. In atypical hemolytic uremic syndrome, there is no preceding diarrhea, so it’s also known as diarrhea negative, or D- HUS.
Additionally, in both types, there can be weakness, fatigue, and vomiting; and hemolysis can cause jaundice, as RBCs are destroyed and bilirubin is produced, and pallor, if anemia sets in. Because of thrombocytopenia, there can be easy bleeding, bruising, petechiae or purpura. Kidney injury causes oliguria or anuria, electrolyte imbalances, as well as edema, most often of the feet, ankles or legs.
Now, the diagnosis of HUS starts with the client’s history and physical assessment. Lab work includes a CBC, which can reveal anemia and thrombocytopenia. With hemolytic anemia, lab tests also show increased bilirubin, which is produced by the metabolism of hemoglobin, and lactate dehydrogenase, which is an enzyme released from the breakdown of RBCs. Schistocytes or helmet cells, which are RBC fragments, can also be found on a blood smear; while a negative Coombs test can help differentiate HUS from other causes of hemolytic anemia. Renal function tests can reveal elevated levels of serum urea and serum creatinine; and urinalysis can show hematuria and proteinuria which are signs of kidney damage. There could also be increased inflammatory markers, like CRP. Finally, with typical HUS, a stool sample can be taken for culture to check for the presence of E. coli or Shigella.
Treatment of HUS should be started promptly to prevent kidney injury, and can include hydration with IV fluids; hemodialysis for clients with acute kidney injury; and transfusions for severe anemia. The toxin usually clears out of the body over a matter of days to weeks. Of note, antibiotics are usually not indicated for typical HUS, as killing the bacteria can result in increased toxin release and worsening of the condition. On the other hand, atypical HUS usually has a worse prognosis, and treatment usually requires identifying and addressing the underlying cause.