Hip fractures: Nursing
Hip fractures: Nursing
Watch later
Watch later
Notes
| HIP FACTURES | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Hip fractures are fractures that occur in the upper third of the thigh bone, called the femur. These fractures can be grouped into two types: intracapsular fractures, which are fractures that happen within the capsule of the hip joint; and extracapsular fractures, which are fractures that happen outside the capsule. One of the most common sites for a hip fracture is at the femoral neck and this is a type of intracapsular fracture.
Now, the hip joint, also called the acetabulofemoral joint, is a ball and socket joint formed between the acetabulum of the hip bone and the head of the femur. The articulating bones are covered by hyaline cartilage and a joint capsule, which is reinforced on the outside by strong ligaments. This makes the joint strong and stable, allowing it to connect the free bones of the lower limb to the pelvic bones. The hip joint allows multiaxial movements, but is also important for weight-bearing and providing stability.
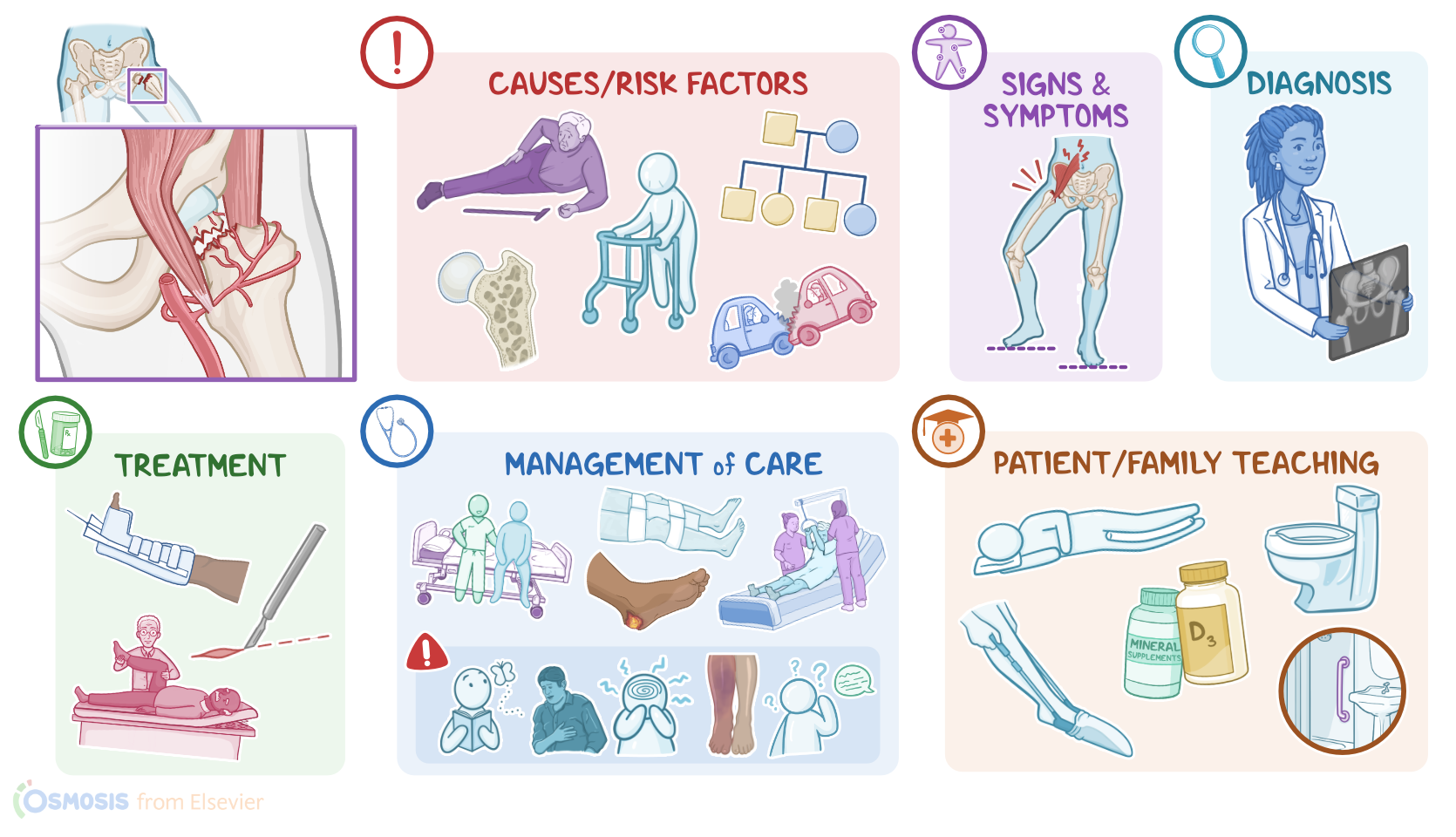
Now, intracapsular fractures are caused by trauma and osteoporosis. Low bone mass due to osteoporosis causes the bones to become more fragile, making them more prone to breaking. Because of this, intracapsular fractures are also called fragility fractures, because they typically occur after minimal trauma, like falling from a chair. On the other hand, extracapsular fractures are typically caused by severe direct trauma, like a car crash.
Risk factors for hip fractures include old age, which can lead to falls, being assigned female at birth, and having a family history of osteoporosis.
Now, the main blood supply for the femoral head comes from the lateral femoral circumflex artery that travels along the femoral head. This artery is often compromised during a hip fracture which can cause complications like avascular necrosis of the femoral head. Furthermore, reduced blood flow means slower healing which leads to longer periods of immobility and hospitalization. This increases the risk of developing thrombotic complications, like deep vein thrombosis and pulmonary emboli as well as other complications like infections.
Clients with a hip fracture typically experience severe pain and tenderness around the affected area which makes it difficult to bear weight on the affected leg. Sometimes, abduction and external rotation of the hip joint, muscle spasm, and shortening of the affected limb might be seen.
The diagnosis of hip fractures starts with the client's history and physical assessment, followed by imaging tests. These include anteroposterior and lateral plain X-rays.
The treatment of hip fractures includes acute management followed by rehabilitation. Acute management includes controlling pain using a regional nerve block, immobilization of the hip joint. Buck’s traction, which keeps the leg in an extended position, is sometimes used. Often, surgical repair and stabilization of the displaced bones is required. Anticoagulants may also be administered to prevent thrombosis and avascular necrosis.
Now, rehabilitation can take place in a rehabilitation unit, a skilled nursing facility, or at home, and consists of physical and occupational therapy. Physical therapy involves early, frequent exercises that restore strength and tone of hip muscles, whereas occupational therapy helps with activities of daily living. Alright, let’s look at the nursing care you’ll be providing for a client with a hip fracture. Your priority goals of care are to prepare your client for surgery, monitor for postoperative complications, and promote mobility.
Begin preparing your client for surgery by immobilizing the affected extremity and helping them into a comfortable position. Assess their pain level and manage their pain by assisting with the insertion of a catheter nerve block and administering a bolus injection of a local anesthetic like bupivacaine, as prescribed. Establish IV access and administer the prescribed prophylactic antibiotic.
After surgical repair, provide standard post-operative care and monitor them closely for complications related to the procedure. Institute fall precautions, maintain bed rest with the affected extremity immobilized and abducted in the prescribed position, and ensure that the head of the bed is not elevated more than 45 degrees to prevent excessive hip flexion. Also continue IV fluids and antibiotics, and manage their pain, as needed. Routinely assess their vital signs and surgical dressing, reinforcing it as needed. Report to the healthcare provider if you notice signs of infection, excessive discharge or bleeding from the wound; as well as the development of fever, hypotension, or tachycardia.
Remember to be vigilant about the prevention of pressure injuries by ensuring your client is placed on a pressure-redistributing surface, monitoring their pressure points, and assisting with position changes at least every 2 hours. Also, encourage them to use the overhead trapeze bar to shift position as needed.