Large for gestational age (LGA) infant: Nursing
Notes
| LARGE FOR GESTATIONAL AGE (LGA) INFANT | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Large for gestational age or LGA for short, is a term used to describe an infant, whose weight is over the 90th percentile for gestational age. In other words, the infant weighs more than 90% of infants of the same gestational age.
Large for gestational age is not a synonym for macrosomia, which is a term used to describe an infant's birth weight over 4000 grams regardless of gestational age. Infants who are LGA can be preterm, term, or postterm.
Now, first, let’s cover some basic physiology.
Gestation refers to the period between conception and birth, which typically lasts for 40 weeks. During these 40 weeks, the embryo, and later fetus, grows and develops within the uterus.
On the other hand, gestational age is a term used to describe a newborn based on their physical and neuromuscular characteristics.
Now, based on the gestational age and the infant’s birth weight, we can determine birth weight percentiles.
The birth weight percentile helps us evaluate the infant’s intrauterine growth and development, which is considered normal when the value is between the 10th and 90th percentile.
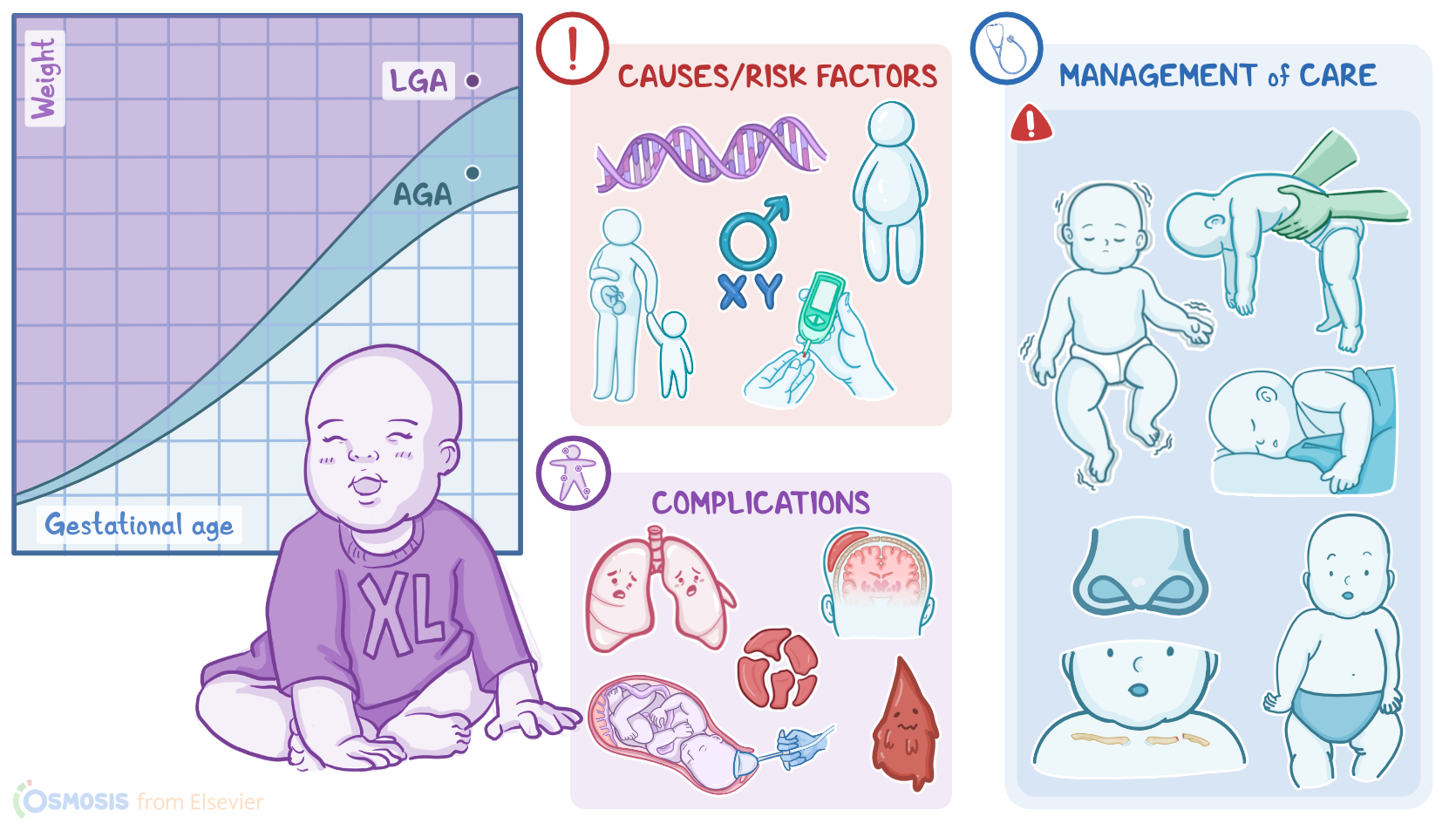
For example, an infant weighing around 3350 grams is within the 40th percentile, and is considered appropriate for gestational age, or AGA. On the other hand, an infant weighing around 2700 grams is within the 3rd percentile, and therefore SGA. Finally, an infant weighing around 4200 grams is within the 95th percentile and is considered large for gestational age, or LGA for short.
Ok, now, when it comes to causes, some LGA infants can be genetically predisposed to be physiologically large; while others have impaired fetal development due to some other fetal or maternal condition.
Important risk factors can be either fetal or maternal risk factors.
A fetal risk factor is male sex. Also, LGA infants are more common in Asian, Black, and Hispanic ethnic groups.
Maternal risk factors include diabetes mellitus, large stature; obesity or excessive weight gain during pregnancy; advanced age; multiparity; and birth of a previous LGA infant.
Now, let’s switch our focus to pathology.
With maternal diabetes, large amounts of glucose are transferred from the mother to the fetus. Unlike glucose, maternal insulin does not cross the placental barrier, so the excessive glucose in the fetal blood signals the fetal pancreas to release more and more insulin, resulting in hyperinsulinemia.
High levels of insulin interfere with normal lung development and decreases surfactant production. Hyperinsulinemia also increases the metabolic rate of the fetus which increases the need for oxygen, increasing the risk of fetal hypoxia.
Hypoxia stimulates erythropoiesis or increased production of RBCs, which ultimately leads to polycythemia. The excess glucose in the fetal blood also increases fat deposits in the subcutaneous tissues and other organs like the liver, heart, and muscle. This causes the fetus to grow much larger than normal, resulting in neonatal macrosomia, meaning that the newborn weighs 4,000 g or more.
Next up are complications, which can be neonatal, maternal, or delivery complications.
Now, for neonatal complications hypoglycemia is one of the most common. This is because, after delivery, the newborn’s insulin level remains high, but the supply of glucose is abruptly cut off when the umbilical cord is cut, leading to hypoglycemia.
Other complications include birth injuries due to macrosomia, since the larger body size makes vaginal delivery more difficult, and increases the risk for trauma during birth, including brachial plexus or facial nerve injury; clavicular, humeral, or skull fractures; cephalohematoma, which is a collection of blood between the periosteum and the skull; as well as subdural hemorrhage.
Respiratory distress is another common complication, which can occur because of lung immaturity; and polycythemia-related problems can also occur, like hyperbilirubinemia, caused by the breakdown of an increased number of circulating red blood cells; as well as hyperviscosity, which can lead to a sluggish blood flow, ischemia, and thrombosis of vital organs.
In some cases, perinatal asphyxia and meconium aspiration may occur. There are also maternal complications, the most common of which include uterine rupture; perineal and vaginal tears; and postpartum hemorrhage.
Finally, delivery complications primarily include the use of operative delivery methods such as vacuum extraction, forceps, or Cesarean birth; and there is a higher risk of shoulder dystocia, meaning the fetal shoulders can’t progress past the maternal pubic bone after the fetal head has been delivered.
Now, let’s switch gears and move on to clinical manifestations. Large for gestational age infants are typically lethargic, obese, have a plethoric appearance, and often feed poorly.
The infant could be jittery due to hypoglycemia; and they often have signs of respiratory distress like tachypnea.
If a cephalohematoma is present, there will be a soft swelling on the skull with defined margins that don’t cross suture lines.
Injury to the facial nerve can be noted if there are asymmetrical facial movements, or if the eye on the affected side doesn’t close completely when the infant cries.
Other clinical manifestations include a limp, adducted, and internally rotated arm if brachial plexus injury is present; decreased movement of the affected side if there’s a humeral; or crepitus, which is a grinding feeling on palpation, if there’s a clavicular fracture.