Multiple myeloma: Nursing
Multiple myeloma: Nursing
Patho 2 Exam 4
Patho 2 Exam 4
Notes
| MULTIPLE MYELOMA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Multiple myeloma, also called plasma cell myeloma, is a condition in which there’s a malignant proliferation of plasma cells in the bone marrow. This further affects the bones and eventually destroys them.
First, let’s look at the physiology of the bone marrow and plasma cells. The main function of the bone marrow is to transform hematopoietic stem cells into all types of blood cells, like red blood cells, platelets, and white blood cells, which include lymphocytes. Plasma cells, specifically, develop from B-lymphocytes, or B-cells, which are key cells of the adaptive immune response. In the bone marrow, B-cells mature and acquire a set of diverse B-cell receptors. Afterwards, they are sent to the lymphoid tissue, like the lymph nodes and the spleen, where they encounter various antigens. By meeting different types of antigens, B-cells are activated and specialize into antibody-secreting plasma cells that are able to fight off infections.
Now, the cause of multiple myeloma is still unknown. However, some evidence suggests that genetic abnormalities in oncogenes, which are genes involved in the uncontrolled proliferation of cancer cells, can play a role in the development of multiple myeloma.
However, there are some known risk factors for developing multiple myeloma, which include age above 60 years old; a past medical or family history of plasma cell tumors; exposure to radiation or organic chemicals, like benzene, herbicides and insecticides; as well as some professions with increased exposure to environmental toxins, like firefighters. Finally, viral infections that impair the immune system, like an HIV infection, are also a risk factor for multiple myeloma.
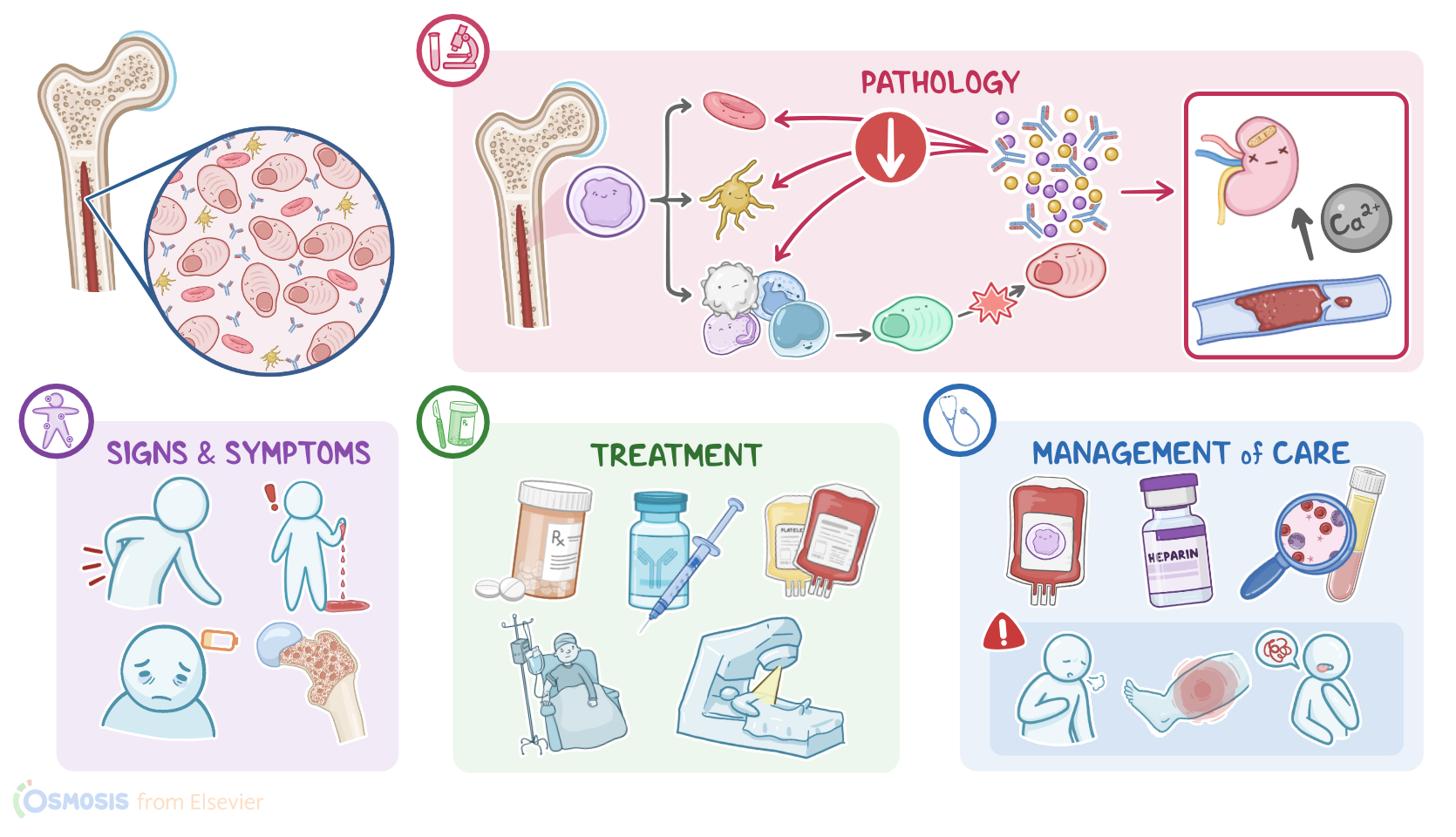
Okay, now let’s look at the pathology of multiple myeloma, which starts with excess production of abnormal plasma cells in the bone marrow. These abnormal plasma cells produce monoclonal antibodies, called M proteins, which are ineffective at fighting off infections. Some of the M proteins accumulate in the bone marrow. and lowers the production of normal red, white cells and platelets, resulting in pancytopenia. At the same time, when abnormal plasma cells proliferate, it reduces the number of normal plasma cells, which affects the body’s natural immune response even more, so there’s an increased risk of infections. Some monoclonal antibodies are released into the blood where they can cause end organ damage. Bence-Jones protein, which is the light chain portion of the M protein, can accumulate in the kidneys and cause renal damage.
On the other hand, excess plasma cell production also leads to increased production of proinflammatory cytokines, like interleukins, that play a role in bone destruction. Bone destruction leads to hypercalcemia and pathological bone fractures. Abnormal plasma cells can also make their way into the circulation, where they can cause hyperviscosity syndrome, meaning unusually thick blood, which poses a high risk of thrombosis. Now, let’s switch gears and look at the clinical manifestations of multiple myeloma. Remember that this condition develops slowly, so in early stages, there’s often no symptoms; therefore this phase is sometimes also called “smoldering” multiple myeloma. Active multiple myeloma is when symptoms develop, with the most common symptom being skeletal pain, which usually affects the lumbar spine, but can also affect the pelvis or ribs. Clients can also develop osteopenia and fractures, as well as signs and symptoms of hypercalcemia, including anorexia, confusion, constipation, polyuria, or cardiac arrhythmias. Sometimes, there can be signs of spinal cord compression like back pain, decreased height, weakness, numbness or dysesthesias in the extremities.
As a consequence of pancytopenia, the client can present with fatigue, malaise, frequent infections or bleeding. Hyperviscosity syndrome is classically associated with a triad of findings that include spontaneous bleeding, commonly from the nose and gums, visual disturbances such as blurry vision or vision loss, and neurological findings like headache, confusion and peripheral neuropathy. Sometimes, signs and symptoms of heart failure can also occur.
The diagnosis of multiple myeloma starts with the client’s history and physical assessment. Lab tests include a complete blood count which shows pancytopenia. Biochemistry tests show hypercalcemia and a high level of M proteins. When the kidneys are also affected, there’s a high creatinine level and the urine sample shows the presence of light chain M proteins. Normally, the serum kappa/lambda ratio is between 0.26 and 1.65. With multiple myeloma, this ratio is usually abnormal, so either lower or higher than normal. Additionally, when the ratio is over 100, that signifies a risk of end-organ disease associated with multiple myeloma.
Other tests include a bone marrow biopsy, which shows excessive monoclonal plasma cells. Imaging studies such as a whole-body CT, MRI or PET scan, can identify osteolytic bone lesions, fractures or bone marrow infiltrations.
Finally, the diagnosis of active multiple myeloma is based on the CRAB criteria, where C stands for hypercalcemia, R stands for renal failure, A stands for anemia, and B for the presence of bone lesions.
Treatment of multiple myeloma involves prophylaxis of bone fractures with bisphosphonates, which can also help with bone pain. Supportive management includes treating anemia or pancytopenia using blood and platelet transfusions or erythropoietin-stimulating factors. However, the ultimate goal of management is to slow down the disease progression. This can be done using corticosteroids, chemotherapy, radiotherapy, or immunotherapy. Finally, hematopoietic stem cell transplantation can be done, and surgery can be necessary for complications like fractures or bone compression.
Alright, let's discuss the management of care for a client with multiple myeloma. Your goals of care include providing supportive care for disease-related symptoms and managing pain.
Now, as you provide care, keep in mind that your client is at a higher risk of developing fractures, so begin by instituting fall precautions, and provide skeletal support when you are assisting them with position changes or ambulating. Next, perform a pain assessment to determine the location, quality, severity and timing of the pain as well as any factor that provokes or relieves their pain. Administer the prescribed analgesic as well as a bisphosphonate to help slow bone damage in addition to reducing bone pain.