Obsessive-compulsive disorder (OCD): Nursing
Notes
| OBSESSIVE-COMPULSIVE DISORDER (OCD) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
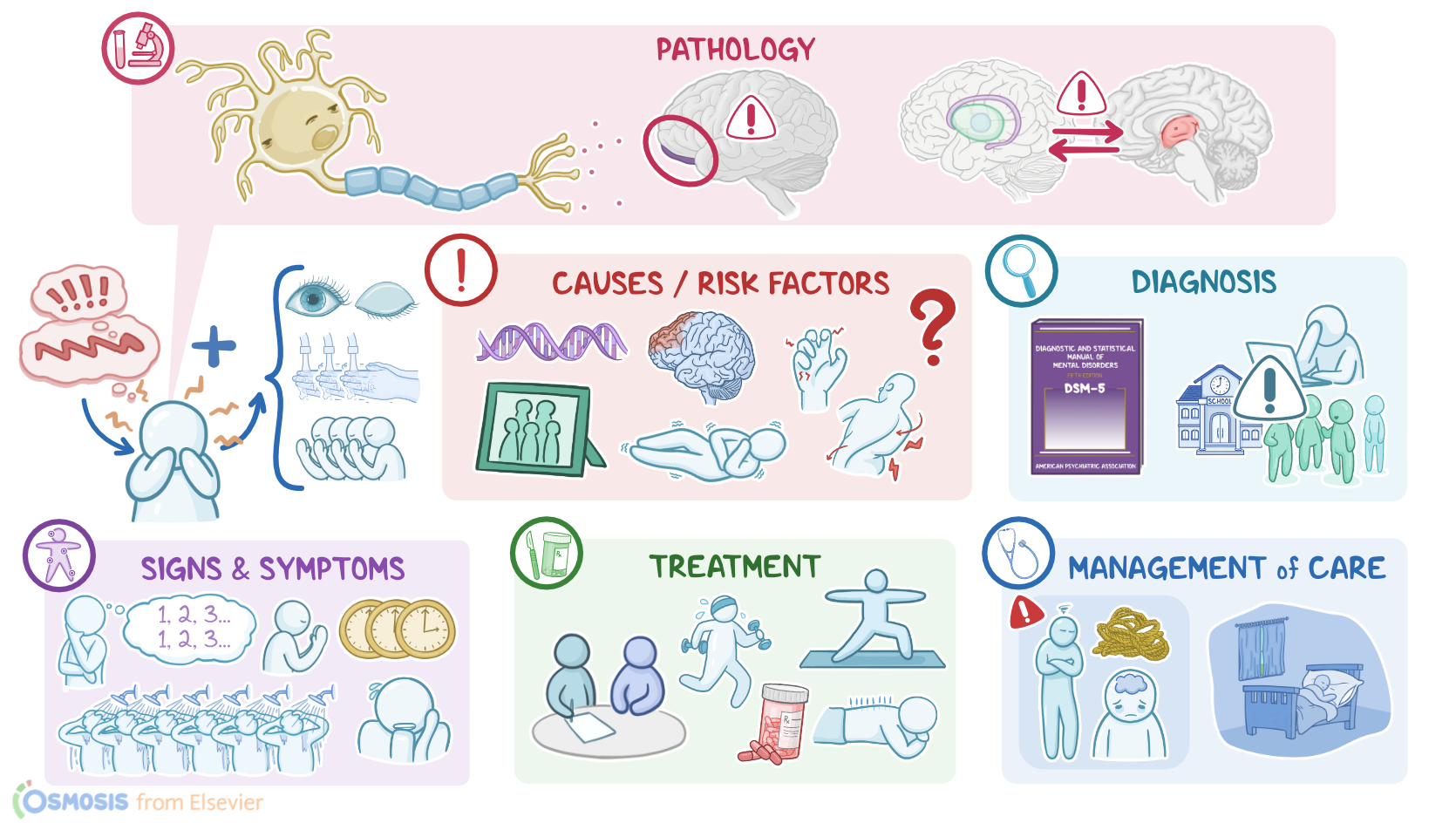
Obsessive-compulsive disorder or OCD for short, is a mental health condition characterized by the presence of obsessions, which are recurrent and intrusive thoughts that can often cause anxiety; and compulsions, which are actions that might be performed to try to reduce the anxiety associated with obsessions.
Now, let’s go over some physiology. Within the brain, there are many different types of neurons that communicate with each other with small molecules called neurotransmitters. Neurotransmitters include serotonin, dopamine, and norepinephrine, which are released from one neuron and bind to receptors of another neuron to modulate its activity.
Now, neurons that synthesize and release the neurotransmitter called serotonin are also known as serotonergic neurons and they are involved in the regulation of mood, sleep, appetite, and reproductive behavior. Serotonin is also important for the normal functioning of the corticostriatal-thalamocortical pathway or CSTC for short, which is an important brain pathway that connects the cortex with deeper structures of the brain, such as basal ganglia and thalamus. Moreover, the corticostriatal-thalamocortical pathway helps regulate habits, movement execution, and reward behavior.
Now, even though the exact cause of obsessive-compulsive disorder remains unknown, what is known is that risk factors include genetic predisposition; family history, and the presence of neurological conditions, like Huntington chorea, brain trauma, and epilepsy.
Now, the pathology of obsessive-compulsive disorder is also poorly understood, but there seems to be a dysfunction of serotonergic neurons, affecting the activity of the corticostriatal-thalamocortical pathway. As a result, normal communication between the cortex and deeper brain structures is impaired. Also, it’s thought that there’s also some kind of dysfunction in the orbitofrontal cortex, which is a part of the brain that’s responsible for switching from habitual to goal-directed behavior.
Now, moving on to clinical manifestations, obsessive compulsive disorder typically presents with obsessions and compulsions that may cause significant impairment at school, work, or social life.
Obsessions are persistent, repeated, unwanted thoughts, urges, or mental images that cause anxiety or distress. For example, a client at a restaurant can’t stop thinking about how the waiter’s hands are covered in germs, so the plate of food in front of them is covered in germs, the utensils and napkins are covered in germs, and so on. These obsessive thoughts are hard to get rid of and usually disappear only after performing a certain action or series of actions called compulsions.
Compulsions are most commonly repetitive ritualistic actions like hand washing and eye blinking, or mental acts such as praying, counting, or repeating words silently. Compulsions are often illogical, like counting the numbers on a clock 3 times before going to work to avoid being late; or excessive, like showering 6 times a day. The client feels driven to perform these actions because it’s the only way to relieve their anxiety or distress despite the fact that they know the actions are illogical or excessive in nature.
Diagnosis of obsessive-compulsive disorder is based on detailed history and physical assessment. Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a mental health condition. So, the first diagnostic element for obsessive-compulsive disorder is the presence of obsessions or compulsions or both. Secondly, these obsessions and compulsions must be time-consuming, take up more than an hour per day, and should cause significant distress. Usually, they repeat themselves to the point where the client is unable to function in school, work, or in personal relationships. Finally, the symptoms shouldn't be caused by a substance, medication, or another medical condition.
Treatment of obsessive compulsive disorder mainly involves non-pharmacological therapy. This consists of psychotherapy, including cognitive-behavioral therapy, which focuses on teaching the client strategies to identify exaggerated patterns of thinking and obsessive thoughts, and then challenge them efficiently. In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Pharmacological therapy, on the other hand, can be used in addition to non pharmacological measures if those alone don’t control the disorder. These mainly include selective serotonin reuptake inhibitors, like sertraline, and antipsychotics, such as risperidone. Also, experimental work has suggested a role for deep brain stimulation in obsessive-compulsive disorder, where a neurostimulator or a “brain pacemaker” is implanted in the brain to send electrical impulses to specific targets in the brain nuclei.