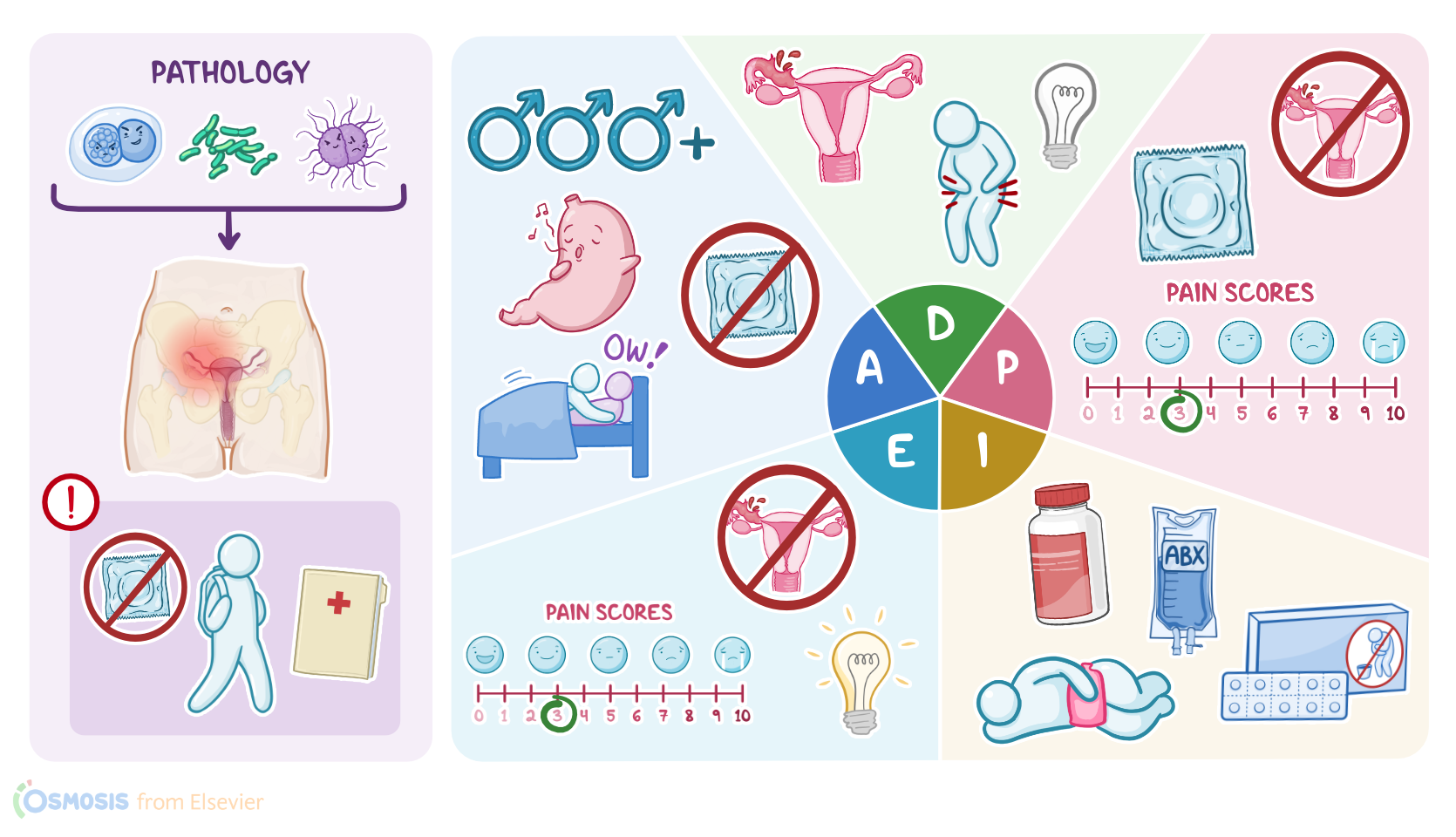
Pelvic inflammatory disease (PID): Nursing process (ADPIE)
Client Report0:00–0:58
Margarita Salvador is a 25-year-old female client who presents to her gynecologist’s office with a report of lower abdominal pain, a fever of 101°F or 38.3°C, chills and thick, yellow foul smelling vaginal discharge.
She states her symptoms began three days ago. A pelvic examination is positive for cervical motion tenderness and right-sided adnexal tenderness.
A transvaginal ultrasound visualizes a 4 cm right-sided tubo-ovarian abscess. A vaginal swab was sent for laboratory analysis to check for chlamydia and gonorrhea.
Ms. Salvador is diagnosed with pelvic inflammatory disease, or PID, and will be admitted to the medical surgical unit for treatment.Pelvic inflammatory disease, or PID for short, is an infection of the upper female reproductive system, which includes the uterus, fallopian tubes, and ovaries.
Pathology0:58–5:04
Most often, PID develops from a bacterial infection that begins in the vagina or cervix, such as sexually transmitted infections, or STIs, like chlamydia, caused by Chlamydia trachomatis, and gonorrhea, caused by Neisseria gonorrhoeae.
Another cause of PID can be bacterial vaginosis, which refers to the infection of the vagina due to overgrowth of bacteria like Gardnerella vaginalis, which are normally present in low numbers in the vaginal flora.
Occasionally, PID can be caused by other forms of bacteria introduced in the reproductive tract during surgery, abortion, or even childbirth.
Now, PID is typically caused by only one type of bacteria, but in some clients, the infection can become polymicrobial, meaning the original infection makes it easier for other bacteria to settle into the reproductive tract.Risk factors associated with pelvic inflammatory disease can be subdivided into two main groups.
Modifiable risk factors include having unprotected sexual contact, as well as new or multiple sexual partners. On the other hand, non-modifiable risk factors include being under the age of 35, since they’re more likely to have new or multiple sexual partners, as well as having a history of prior pelvic inflammatory disease, STIs, or bacterial vaginosis.Some clients with PID will have no or mild symptoms.
On the other hand, symptomatic clients may present with fever, pelvic pain, and tenderness around the ovaries and fallopian tubes, as well as dyspareunia, which is pain during sexual intercourse.
Additionally, some may complain of mucopurulent vaginal discharge or irregular uterine bleeding. Pelvic inflammatory disease can cause some serious complications, such as adhesions and strictures of the fallopian tubes, subsequently increasing the risk of ectopic pregnancy and infertility.
In addition, if pus builds up in a tube and ovary, it can turn into a tubo-ovarian abscess, which can rupture and spread into the bloodstream, leading to sepsis.
Finally, if the inflammation affects the peritoneum and Glisson’s capsule surrounding the liver, it can result in strings of scar tissue that attach the liver to the peritoneum.
These “violin string” adhesions are also known as Fitz-Hugh-Curtis syndrome, which is also called perihepatitis. Diagnosis of PID is usually based on history and clinical findings, such as pelvic pain and cervical motion tenderness, which refers to the pain and discomfort that occurs during mobilization of the cervix.
In some clients, the cervix can also be inflamed, erythematous, and bleed easily when touched. In addition, it’s important to check blood levels of beta human chorionic gonadotropin, or beta hCG for short, and perform an ultrasound to rule out pregnancy.
Ultrasound can also help visualize complications like a tubo-ovarian abscess. Next, a swab sample from the inside of the vagina or cervix can be tested for chlamydia and gonorrhea, using the nucleic acid amplification test or NAAP for short.
Finally, urinalysis can be performed to rule out urinary tract infections that might present with similar clinical findings.
Clients with pelvic inflammatory disease are typically treated with a mix of antibiotics, including ceftriaxone or cefotetan, doxycycline, and metronidazole.
Additionally, analgesics like acetaminophen or NSAIDs can be used to manage pain. Some clients might require surgery to remove adhesions or treat complications.Now, let’s get back to Ms.
Assessment5:04–6:57
Salvador and begin her assessment. As you enter her room you note Ms.
Salvador appears uncomfortable and is guarding her lower abdomen. While reviewing her history, she tells you she has had several male sexual partners in the past and no female sexual partners.
She does not routinely use protection and last had intercourse two days ago, which she recalls as being painful. Her last menstrual cycle ended 5 days ago.
Her vital signs are: temperature 101.2°F or 38.4°C, heart rate 100 beats per minute and regular, respirations 18 breaths per minute, blood pressure 126/82 mmHg, and oxygen saturation 98% on room air.
Her oral mucous membranes are moist and pink. Capillary refill is less than 3 seconds, and peripheral pulses are 3+ and equal bilaterally.
Ms. Salvador’s bowel sounds are active, and she denies nausea, vomiting, or changes in bowel movements.
Reviewing her lab results, you note the following: leukocytes 14,000/mm3; erythrocyte sedimentation rate 40 mm/h; beta hCG 1.0 IU/L; urinalysis is positive for WBCs with no organisms present.
Salvador know you will be back to check on her shortly.OK, you’ve gathered assessment data so now you develop nursing diagnoses for Ms.
Salvador, which include: risk for infection related to potential for abscess to rupture and sepsis; acute pain related to pelvic inflammation; and ineffective health maintenance related to deficient knowledge regarding prevention and treatment of STIs.
Diagnosis6:57–7:18
Alright, with nursing diagnoses in place you’re ready to plan goals for Ms. Salvador.
By the end of your shift, Ms. Salvador will exhibit no signs of a ruptured abscess or sepsis; she will achieve pain control at her stated tolerable level of 3/10; and she will demonstrate understanding of PID and ways to prevent STIs.Implementing your plan with the help of the interdisciplinary team is the next step in caring for Ms.
Planning7:18–7:39
Salvador. After reviewing orders placed by the physician, you collaborate with the patient care technician, or PCT, and delegate collection of vital signs and intake and output, requesting to be notified immediately of any changes.
Implementation7:39–9:16
To promote drainage of the pelvic cavity, you ensure Ms. Salvador remains in the semi-Fowler position while she is in bed.
Next, you administer the ordered IV antibiotics cefoxitin and doxycycline. Then, you administer the antipyretic acetaminophen, the analgesic tramadol and apply a heating pad to her lower abdomen.During your shift, you teach Ms.
You teach her to recognize the signs and symptoms of infection in herself and her partners, and you let her know that her most recent partners must be assessed and treated as needed.
You further stress the importance of waiting to resume sexual activity until after her antibiotic regimen is completed and her follow-up STI test results are back.
Next, you explain how PID can lead to chronic pelvic pain and cause scarring of her fallopian tubes, which can lead to impaired fertility and increase the risk of ectopic pregnancy.Throughout your shift, you closely monitor Ms.
Salvador for signs of sepsis and increasing pain, knowing these changes warrant urgent physician notification and prompt action.OK, it’s the end of your shift and time to evaluate the effectiveness of the nursing interventions provided to Ms.
Salvador so far. Her latest set of vital signs are: temperature 99.4°F or 37.4°C, heart rate 80 beats per minute, respirations 16 breaths per minute, blood pressure 118/78 mmHg SpO2 99% on room air, and pain 3/10.
Evaluation9:16–10:13
She has warm, dry, intact skin with normal turgor. Ms.
Salvador verbalized her understanding of the education you provided. You are happy to see her pain and fever improving, that she isn’t showing signs of a ruptured abscess or sepsis, and that she has gained new understanding of how she can promote her own sexual health.
You give the report to the next shift so Ms. Salvador’s plan of care can be continued and adjusted as needed.
Alright, as a quick recap... your client, Margarita Salvador, was treated for PID, which is an infection and inflammation of the upper female reproductive system that has resulted in a tubo-ovarian abscess.
Ms. Salvador’s assessment revealed fever, pelvic pain, and vaginal discharge as well as unsafe sexual practices and painful intercourse.
Nursing diagnoses to guide Ms. Salvador’s care included: risk for infection; acute pain; and ineffective health maintenance.
Summary10:13–11:12
Planned goals and interventions implemented for Ms. Salvador focused on treating her infection; managing her pain and fever, monitoring for a ruptured abscess and signs of sepsis, and providing health promotion education.
At the end of your shift, you evaluated the nursing care provided. The interdisciplinary team will continue monitoring Ms.
Salvador and adjusting her plan of care to help her reach the best outcomes possible. infection acute pain, and ineffective, Health maintenance.
Plans goals and interventions implemented for Miss Salvador focused on treating her infection managing, her pain, and fever monitoring for a ruptured abscess and signs of sepsis and providing health promotion education.
At the end of your shift, you evaluated the nursing care provided. The interdisciplinary team will continue monitoring this Salvador and adjusting her plan of care to help her reach the best outcomes possible.
| PELVIC INFLAMMATORY DISEASE (PID) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
No notes for this video yet
Try adding a note below