Meningitis: Nursing process (ADPIE)
Meningitis: Nursing process (ADPIE)
Watch later
Watch later
Notes
| MENINGITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Alejandro Delgado is a 19-year-old college student who was brought to the emergency department, or ED, by his roommate with a report of a sudden onset of headache, confusion and fever.
He has a petechial rash on his arms and chest.
The lesions don’t blanch, and Alejandro says they appeared a few hours before he came to the ED.
Alejandro has no known allergies or comorbidities, and he is not aware that he’s been exposed to someone who is sick.
The ED physician performed a targeted neurological examination which showed nuchal rigidity.
Kernig and Brudzinski signs were negative.
A lumbar puncture and blood draw were completed and sent to the lab for analysis, Gram stain and culture.
Alejandro was then transferred to the inpatient unit for treatment and continued monitoring.
Meningitis refers to inflammation of the meninges, which are three protective membranes that cover the brain and spinal cord.
From outside to inside they’re the dura mater, arachnoid mater, and pia mater, with cerebrospinal fluid, or CSF for short, in the space between the arachnoid and pia.
Now, meningitis can be caused by any pathogen that can infect the meninges, such as viruses, bacteria, fungi, and parasites.
The most common and life-threatening type is bacterial meningitis.
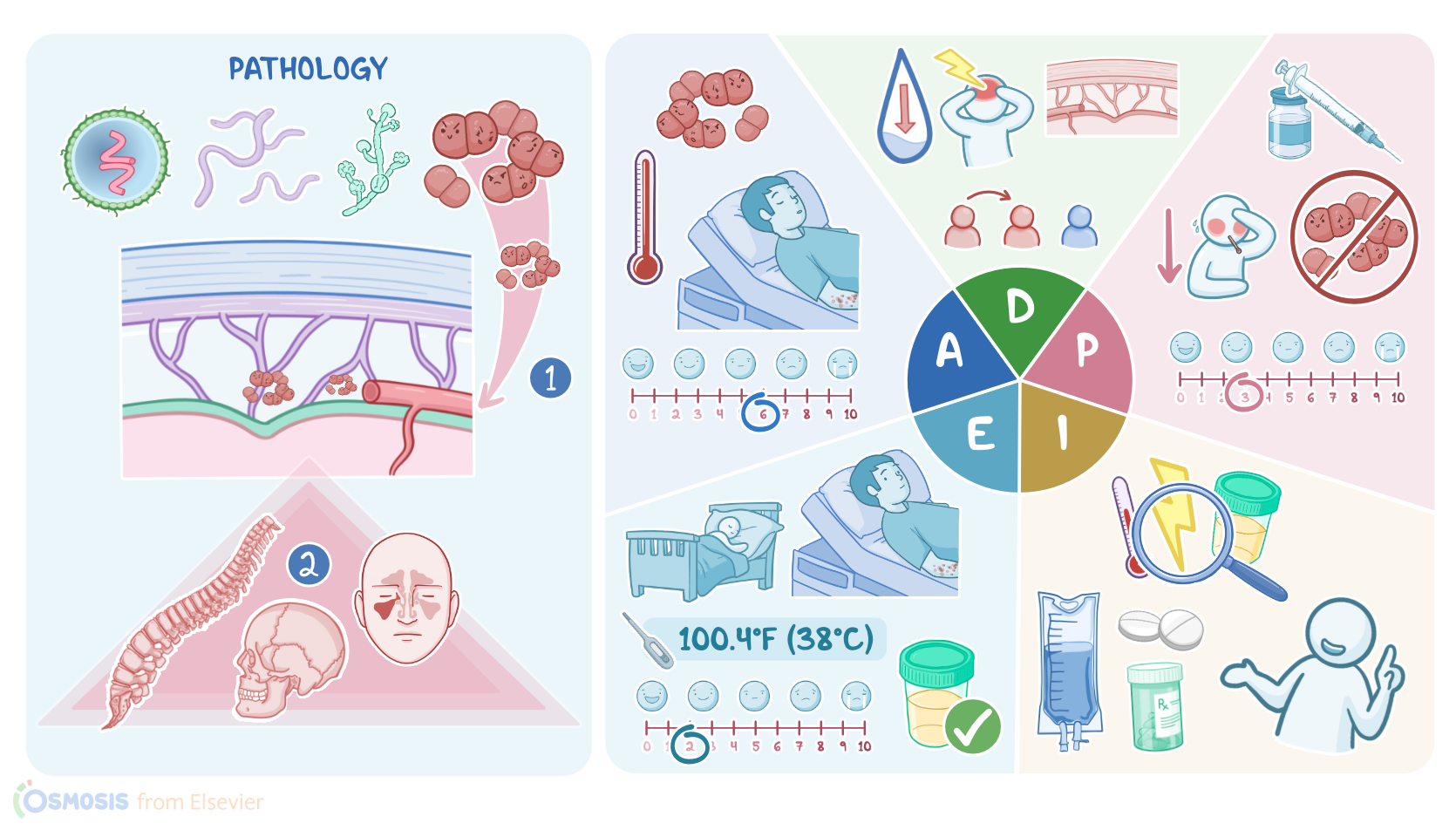
There are two routes that bacteria can use to reach the meninges.
The most common route is hematogenous spread, which is when bacteria enter the bloodstream and move through the blood brain barrier to reach the meninges.
The second way is by direct spread from a nearby infected structure, like the skull, spine, or sinuses.
Bacterial meningitis is more common in clients at the extremes of age, such as children younger than 5 years old or adults who are older than 60, as well as those who have other conditions, such as diabetes, HIV, cirrhosis, chronic kidney disease, malignancy, cystic fibrosis, or a history of splenectomy.
Other important risk factors include nearby infections, such as sinusitis, mastoiditis, and otitis media, as well as having neurosurgery, skull fractures, or congenital defects like spina bifida.
Finally, there’s also increased risk in crowded environments, since some bacteria can be transmitted from person to person and cause outbreaks within households, military barracks or college dorms.
Okay, now the most likely causative bacteria depend on the client’s age group.
In infants younger than 3 months, the most common causes are bacteria that normally can colonize the vaginal mucosa, so the baby can come in contact with them during labor.
This includes group B Streptococci, Escherichia coli, and Listeria monocytogenes.
In children between 3 months to 12 years old, as well as in adults, meningitis is generally caused by bacteria that can colonize the nasopharynx.
Specifically, Streptococcus pneumoniae is the most common cause, followed by Neisseria meningitidis, and Haemophilus influenzae.
Between these two group ages, there’s adolescents between 13 to 17 years old, in which the most common cause is Neisseria meningitidis, which takes more close or lengthy personal contact to spread, such as kissing, followed by Streptococcus pneumoniae, and Haemophilus influenzae.
Vaccines such as the Meningococcal, Pneumococcal, and Hib vaccines can help prevent meningitis caused by these bacteria.
Finally, in adults over the age of 50 or those who are immunocompromised, an important cause is Listeria monocytogenes, since it causes an opportunistic infection that a strong immune system would usually be able to fend off.
Also, in clients of any age group who have a history of neurosurgical procedures or trauma to the head, an honorable mention goes to Staphylococcus aureus, which normally colonizes the skin, so any breaks can allow it to spread.
All right, now meningitis usually presents with a triad of fever, headache, and neck rigidity or stiffness.
Other common symptoms include nausea and vomiting, as well as photophobia or extreme sensitivity to light, and phonophobia or extreme sensitivity to noise.
Upon physical exam, some characteristic signs that indicate meningeal irritation include the Kernig sign, where the client feels pain and spasm in the hamstring when their knee is fully extended from a flexed, 90 degree angle; and the Brudzinski sign, where passively flexing the neck forward triggers pain and an involuntary flexion of the hips.
If untreated, meningitis can lead to complications, which can eventually lead to coma or even death.
One of the main complications is meningoencephalitis, which is when the infection spreads to the brain, and can present with seizures and mental status alterations, such as confusion,
personality changes, drowsiness, and lethargy.
Sometimes, the bacteria can also collect and wall off from the rest of the brain forming a brain abscess.
Another well-known complication is cranial nerve palsy, which is characterized by inflammation and impaired function of one or more cranial nerves; most often, this involves the 8th cranial nerve, which is responsible for hearing and balance, resulting in deafness or dizziness.
Other potential complications of meningitis include stroke, increased intracranial pressure due to cerebral edema, and brain herniation, which is the most common cause of death.
In other cases, bacteria can enter the bloodstream and lead to systemic complications, such as septic shock, and disseminated intravascular coagulation.