Peripheral arterial disease (PAD): Nursing process (ADPIE)
Peripheral arterial disease (PAD): Nursing process (ADPIE)
Watch later
Watch later
Notes
| PERIPHERAL ARTERIAL DISEASE (PAD) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
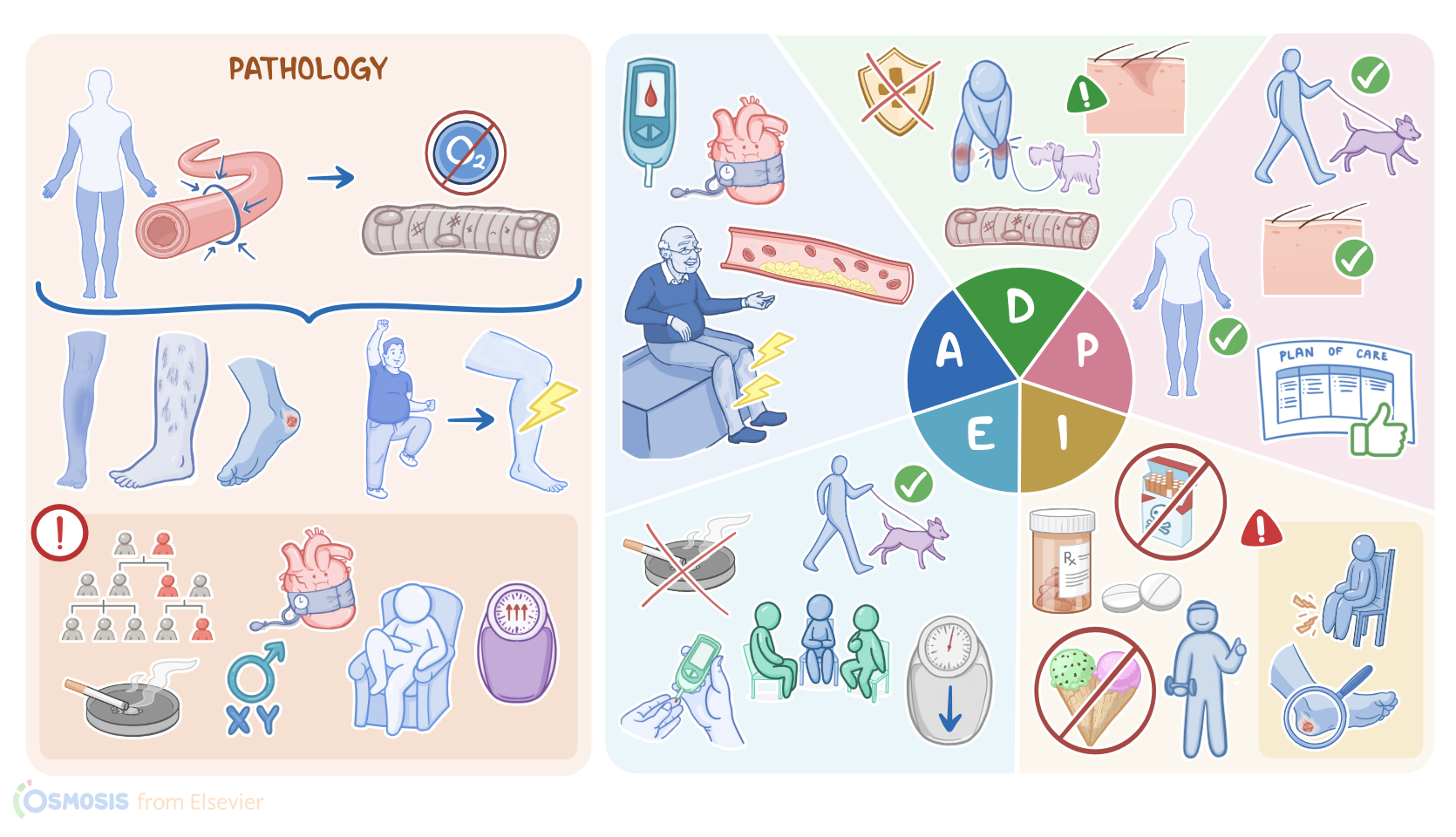
Mike Craig is a 68-year-old male client who is referred to the vascular clinic by his primary care provider, or PCP. Mr. Craig has a history of type 2 diabetes, hypertension, and dyslipidemia, and he’s been experiencing intermittent leg pain in his lower legs while taking walks with his dog.
An ankle-brachial index, or ABI, is performed which confirmed a diagnosis of peripheral artery disease, or PAD. Peripheral arterial disease, or PAD for short, is the progressive narrowing of the arteries that supply peripheral tissues and organs, so basically all arteries except for the heart and brain.
As a result, there’s reduced blood supply to these tissues, which ultimately become ischemic. There are some factors that may put an individual at risk for PAD.
Non-modifiable risk factors include increasing age, male sex, and having a family history of PAD. On the other hand, modifiable risk factors include smoking, obesity, and having a sedentary life, as well as predisposing conditions like diabetes, dyslipidemia, and hypertension.
The most common cause of PAD is atherosclerosis, which is a buildup of fatty and fibrous material just under the inner lining of a blood vessel, forming a plaque.
This buildup usually happens over the course of years. Eventually, the lumen of the vessel becomes so narrow that it results in reduced perfusion to the tissue it tends to supply.
PAD can be worsened by an embolism. This happens when an embolus, which is a piece of blood clot or fatty deposit, breaks off from an atherosclerotic plaque from an upstream artery, and gets lodged in a narrower peripheral artery, blocking its blood flow.
Now, in most cases PAD affects the arteries supplying the legs. When less blood gets to the muscle tissue in the legs, that tissue becomes ischemic, causing a type of cramping pain that is often referred to as intermittent claudication.
Initially though, when the client’s at rest, there’s enough blood to meet the tissue’s demands, so they’ll be asymptomatic. But if the client starts walking or exercising, then the leg muscles start to work harder and demand more blood, which causes the claudication.
In addition, since the muscles aren’t getting enough oxygen from blood, they’ll switch from aerobic to anaerobic metabolism, and the production of lactic acid, which will build up and contribute to the pain.
This is usually felt in the calves, but can also involve the feet, thighs, hips, or buttocks. Other signs and symptoms of PAD include paresthesia, which is described as tingling or numbness, as well as decreased or absent pulses, cool extremities, and atrophy of the muscles.
In addition, clients may present with hair thinning or loss over the affected skin area, as well as skin color changes, which may become pale or bluish, especially when the leg is elevated, which is called elevation pallor.
As the PAD worsens, clients may start experiencing claudication even at rest. The client often describes this as a continuous burning or pain in the forefoot and toes that gets worse when the legs are elevated, and is relieved when they’re lowered, like hanging the feet over the bed, because gravity is working with the blood flow in this direction.
Likewise, the foot might turn red when it’s lowered, which is called dependent rubor. Ultimately, the reduced blood flow can lead to nerve damage, which results in peripheral neuropathy, where the client loses sensation in the affected tissue.
Moreover, the tissue can become necrotic and develop wounds or ulcers that don’t heal, and the limb might be at risk of gangrene and amputation.Diagnosis of PAD relies largely on the client’s history and physical examination.
A quick and noninvasive test is the ankle-brachial index, or ABI for short, where blood pressure is taken in the ankle and in the arm, and then compared. PAD is typically diagnosed if the systolic blood pressure in the ankle divided by the systolic blood pressure in the arm is less than 0.9.
In general, claudication often occurs in clients with an ABI between 0.4 and 0.9, rest pain is seen between 0.2 and 0.4, and ulcers, and gangrene between 0 to 0.4.
Diagnosis of PAD can also involve listening to the pulse in the involved arteries with a stethoscope, so for example in the legs, it would be the iliac arteries. With PAD, the narrowed artery would make a whooshing sound, called a bruit.
Another test that can be done is a doppler ultrasound, which is a way of visualizing blood-flow. Rarely, an angiography might be needed to confirm the diagnosis, by using X-rays and a contrast agent to assess the blood flow in the involved arteries.
Treatment of PAD often requires lifestyle changes that address the underlying risk factors. Clients should quit smoking, lose weight, adopt healthy eating habits, and exercise regularly; as well as managing any associated condition like diabetes and hypertension.
Some clients with PAD can also take certain medications to help reduce blood clotting, such as antiplatelet medications like aspirin or clopidogrel. Clients who fail to respond to these treatments can be treated with revascularization to reestablish arterial blood flow.
Revascularization options include percutaneous intervention or surgical bypass. Finally, clients who present with gangrene require removal of necrotic tissue, and in some cases, the limb would have to be amputated.
Sources
- "Epidemiology and Risk of Amputation in Patients with Diabetes Mellitus and Peripheral Artery Disease" Arterioscler Thromb Vasc Biol (2020)
- "Evidence-Based Medical Management of Peripheral Artery Disease" Arterioscler Thromb Vasc Biol (2020)
- "Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association" Circulation (2021)
- "Antithrombotic Treatment for Peripheral Arterial Occlusive Disease" Dtsch Arztebl Int (2021)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)