Pressure injury: Nursing process (ADPIE)
Client Report0:00–0:31
Joann Mercer is a 78-year-old female client who resides in a skilled nursing facility. Mrs.
Mercer has a history of osteoarthritis and hip fracture. She needs assistance to walk, and spends most of her time in bed or sitting in her wheelchair.
You are concerned that Mrs. Mercer has developed a pressure injury.
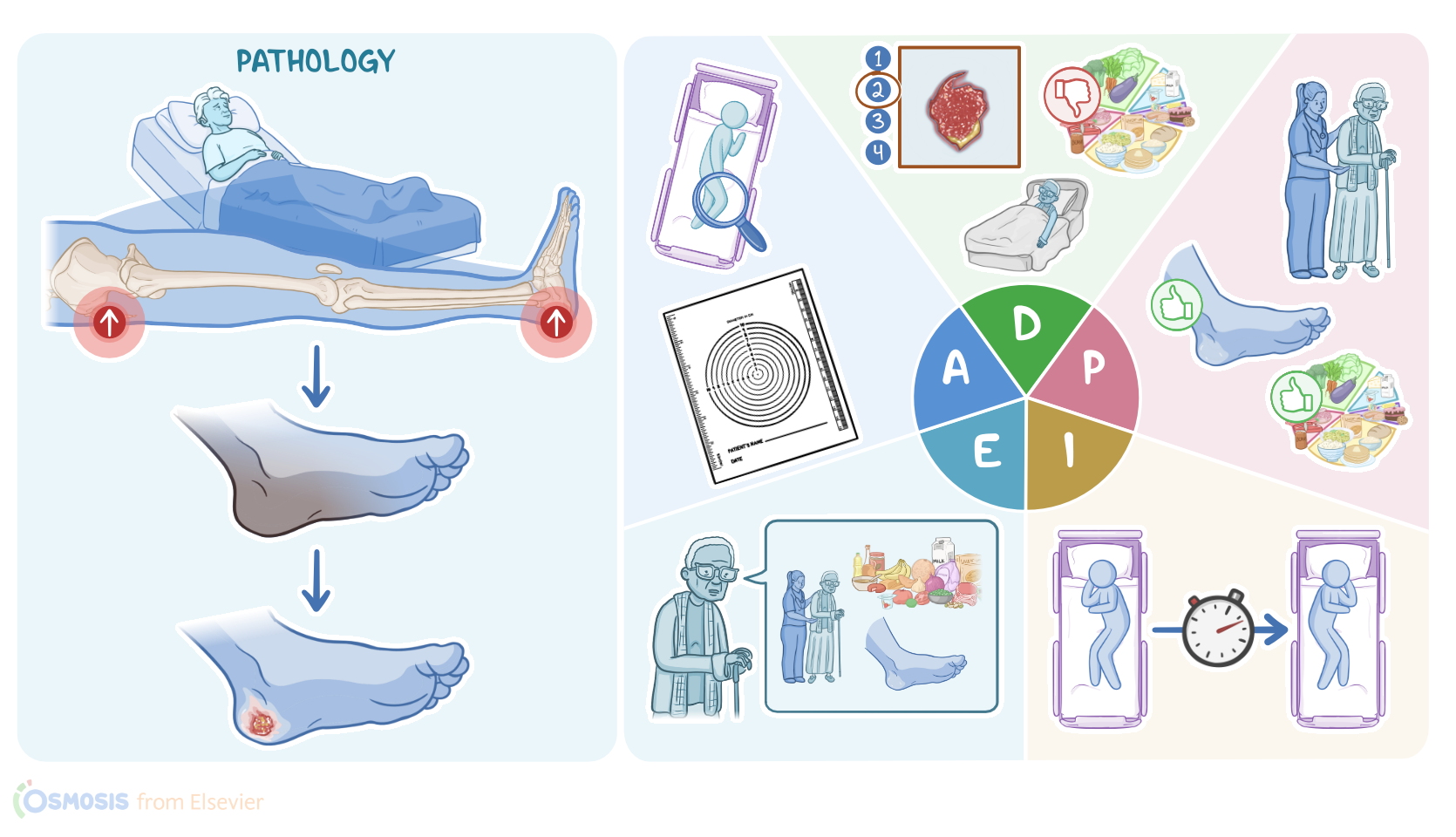
Pressure injuries, also known as decubitus ulcers, involve damage to the skin or underlying tissue that result from prolonged pressure.
Pathology0:31–5:00
Now, pressure injuries usually appear over bony prominences, especially the sacrum, followed by the heels, since these areas have the thinnest subcutaneous tissue between the bone and the skin.
So the prolonged pressure causes a reduced blood flow to that tissue area, resulting in tissue hypoxia and ischemia, and ultimately leading to necrosis and ulceration.
Most often, pressure injuries develop in clients who aren’t moving about, like those on chronic bedrest or consistently in a wheelchair.
Other important risk factors for pressure injuries are conditions that may impair blood flow, such as heart and lung disease and diabetes mellitus.
Clients should be assessed for the risk of developing a pressure injury using a validated assessment tool like the Braden Scale.
This scale looks at six criteria, which include sensory perception, moisture, activity, mobility, nutrition, and friction or shear.
The lower the score, the higher the risk of injury. Nutritional assessments can be used to assess the likelihood of injury as well as healing.
With non-healing injuries, laboratory tests can be done to assess an underlying cause like diabetes or infection. Laboratory tests can include a glucose test, which would reveal hyperglycemia in case of diabetes, or a complete blood count showing elevated white blood cells, an elevated erythrocyte sedimentation rate, and elevated C reactive protein or CRP, as well as blood cultures to check for an infectious cause.
Now, pressure injuries can often cause symptoms like pain or pruritus, and can present with purulent drainage or bleeding.
In addition, pressure injuries can lead to complications like local infections of the wound. In severe cases, the infection may spread and result in bacteremia, which can lead to sepsis, and death.
Pressure injuries are staged according to their level of tissue damage. There are four stages of injury development and pain can present at any stage.
In stage 1 the skin will appear red, but remain intact. When pressed, the area will not blanch or turn white.
At stage 2, there is partial-thickness skin loss, and the wound will look like a shallow open wound or blister. Stage 3 involves full thickness loss of tissue that can present with slough or light-colored dead tissue.
In stage 4, the wound extends deep enough to expose muscle or bone. Eschar, or dark-colored dead tissue, can be present.
Finally, if a pressure injury is completely covered with slough or eschar, it can be difficult to determine its depth; this is referred to as an unstageable pressure injury.
Treatment for pressure injuries depends on the stage of the wound, but generally involves redistribution of pressure, by regularly repositioning the client, as well as ensuring good nutrition and hydration to encourage wound healing; pain management; and frequent monitoring and wound care to keep the wound clean, moist, and covered.
For stage 1 injuries, either a transparent or hydrocolloid type dressing is used. Both are useful in acting as a moisture barrier, as well as preventing shear and friction.
For stage 2 injuries, a hydrocolloid or hydrogel dressing can be used to assist with absorption, protection, and debridement of the wound.
A wet-to-dry gauze dressing can also be beneficial for wound debridement and healing. Stage 4 pressure injuries may need surgical debridement or negative pressure wound therapy to assist healing.
Finally, an unstageable injury may need surgical debridement to properly stage, dress and treat the wound appropriately.
So, after you greet Mrs. Mercer and introduce yourself, you wash your hands, confirm her identity, and begin your assessment by asking her how she’s feeling.
Assessment5:00–6:40
She tells you that she is feeling fine, but hasn’t felt like moving around today. Her vital signs are: heart rate 80 beats per minute and regular; respiratory rate 18 breaths per minute with clear breath sounds bilaterally; blood pressure 124/60 mmHg; temperature 98.4° F or 36.9°C; pain 2/10, which is within her stated level of comfort.
You continue your assessment by completing a full head to toe skin assessment looking for any skin discoloration, redness, or temperature changes.
There is no exudate or odor. You measure the ulcer using a wound measuring card and take a picture to document the wound.
As you review in her chart you note her height 5 feet, 5 inches; weight 110 pounds; and her BMI is 18.3. Previous documentation from 1 month ago shows her weight to be 118 pounds with a BMI 19.6.
Next, you ask Mrs. Mercer about her appetite, and she informs you she often doesn’t feel like eating, explaining that “food doesn’t taste as good as it used to.” You note her most recent Braden score is 12.
Before leaving the room, you assist Mrs. Mercer into a comfortable position with pressure off her wound, and document the stage, size, location of the pressure injury.
Now that you’ve completed your nursing assessment, you establish your nursing diagnosis for Mrs. Mercer: impaired skin integrity related to decreased mobility and presence of a stage 2 pressure injury, imbalanced nutrition: less than body requirements related to insufficient dietary intake, and risk for infection related to an open wound.
Diagnosis6:40–7:02
Now that you’ve formulated your nursing diagnoses, it’s time to develop goals for the plan of care. By the end of the week, Mrs.
Mercer’s wound will show signs of healing, she will ambulate with assistance and change her position regularly, and her dietary intake will improve.
Planning7:02–7:25
During the healing process, your long-term goal is for the wound to remain free from infection. After collaborating with the CNA, the facility’s dietitian, and Mrs.
Mercer, you implement the plan of care. Wound assessment and care will be performed every shift, and if there are any changes to the wound, such as signs of infection, you will notify the supervising physician immediately.
Implementation7:25–8:19
Next, you delegate to the CNA the task of assisting Mrs. Mercer to reposition hourly and ambulate with assistance every 2-4 hours in order to alleviate pressure on her wound and sacrum.
Then, to support healing of her wound, you consult with the facility's dietitian to develop an appealing and nutritious diet plan that incorporates Mrs.
Mercer’s food and beverage preferences. Finally, you spend some time talking to Mrs.
Mercer about how assisting her to increase her activity and eating a healthy diet that includes protein, vitamins, and minerals will help her wound to heal.
Alright, let’s check back in on Mrs. Mercer a week later to evaluate how she is doing.
You assess the wound and dressing and note that the dressing is clean, dry, and intact. Comparing the initial measurement of the wound with today’s measurement, you note a small decrease in the wound’s surface area.
Evaluation8:19–8:49
She tells you she has been ambulating with assistance in the hallway regularly and that she’s been enjoying her new meal plan.
Her weight today is 118.5 pounds. Okay, as a quick recap… Your client, Mrs.
Mercer, currently resides in a skilled nursing facility. Pressure, limited mobility, age, and inadequate nutrition contributed to the development of a stage 2 pressure injury.
Your assessment revealed a shallow open ulcer, with a reddish-pink wound bed, inadequate dietary intake, decreasing weight, and a Braden Score of 12.
Summary8:49–9:47
Your nursing diagnoses included impaired skin integrity, imbalanced nutrition: less than body requirements, and risk for infection.
The planning goals included decreasing pressure on her sacrum, increasing mobility, increasing her dietary intake, and that the wound would begin to heal and remain free of infection.
Along with the health care team, you work to implement interventions to achieve the goals of the plan of care. Throughout your shift, and up until Mrs.
Mercer’s wound heals, you will continue to evaluate and revise your plan of care as needed. healthcare team you work to implement interventions to achieve the goals of the plan of care throughout your shift and up until mrs.
Mercer's wound heals. You continue to evaluate and revise your plan of care
| PRESSURE INJURY | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
No notes for this video yet
Try adding a note below