Schizophrenia: Nursing
Introduction0:00–0:18
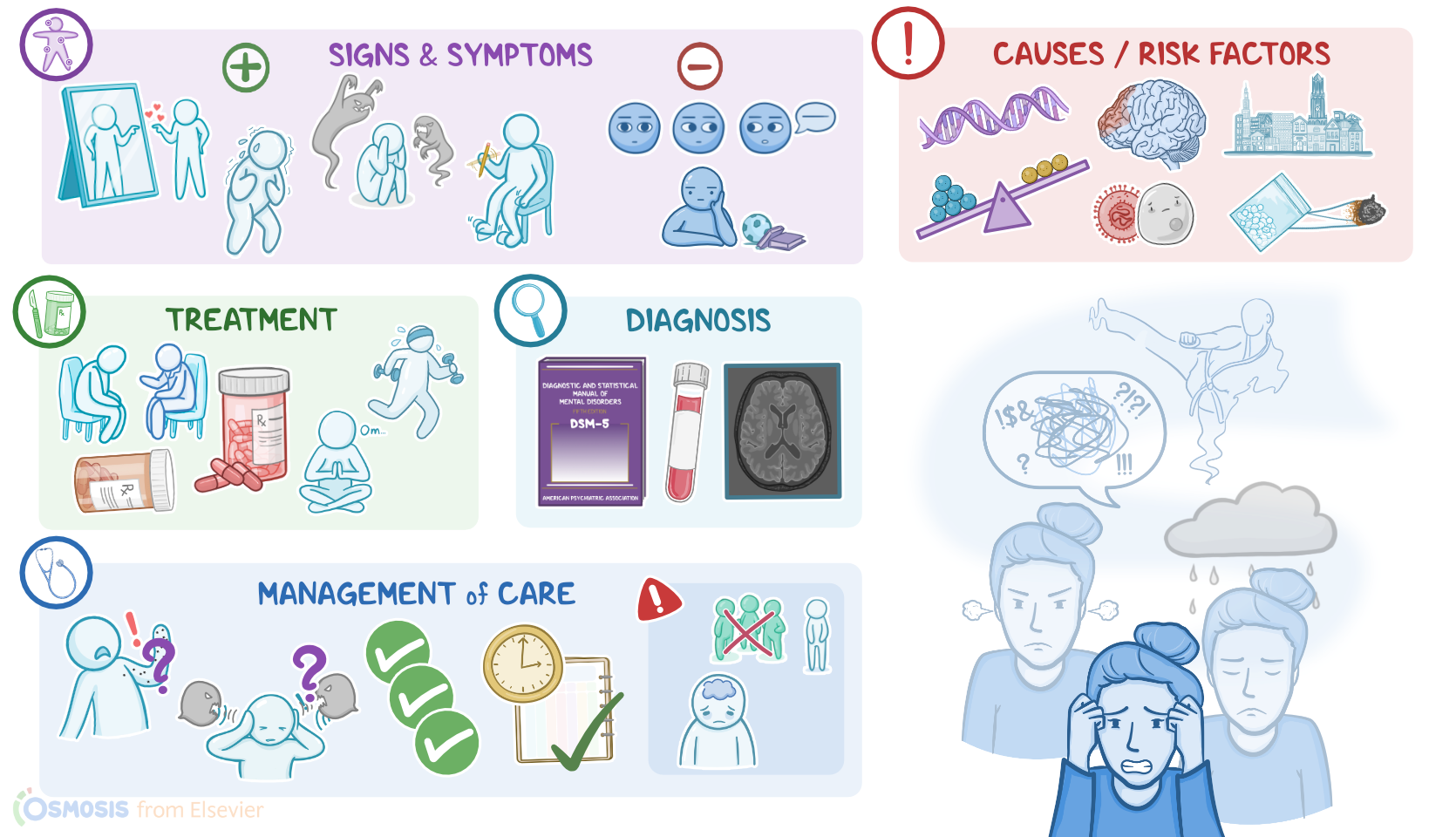
Schizophrenia is a psychiatric condition caused by imbalanced dopamine levels in the brain. It’s characterized by disturbances in perception, thinking, behavior, and emotions.
Alright, now let’s cover some basics of brain anatomy and physiology. Neurons communicate with each other through neurotransmitters.Some, like glutamate, are excitatory neurotransmitters, meaning they cause neurons to fire.
Physiology0:18–1:18
Some, like GABA, are inhibitory neurotransmitters and prevent a neuron from firing.Finally, there are some like dopamine that could be excitatory or inhibitory depending on what neurons they act upon.Dopamine is a neurotransmitter that’s primarily found in 4 main dopaminergic pathways of the brain; the mesolimbic pathway, which controls motivation and desire; the mesocortical pathway, which helps regulate emotions; the nigrostriatal pathway, which helps control voluntary movements; and lastly, the tuberoinfundibular pathway, which releases dopamine to limit the secretion of prolactin.Now, the exact cause why schizophrenia occurs is still not fully understood; but, some theories suggest that it’s due to a combination of neurotransmitter imbalances in the brain, and anatomical brain changes due to genetic and environmental factors during early brain development.
Causes and risk factors1:18–1:59
Now, the main risk factors for developing schizophrenia include genetic predisposition, having a family history of schizophrenia; perinatal complications like infections, hypoxia, living in urban areas; as well as exposure to toxins; and the use of substances, especially cannabis, LSD, and methamphetamines.Now, the mechanisms underlying the pathology of schizophrenia are poorly understood, but there seems to be abnormal levels of dopamine, particularly in the mesolimbic and mesocortical pathways.
Pathology1:59–2:43
So, high levels of dopamine in the mesolimbic pathway result in positive symptoms, while low levels of dopamine in the mesocortical pathway cause negative symptoms.Another contributor to the negative symptoms is the decreased activity of excitatory neurons throughout the brain that use glutamate as the neurotransmitter.
Finally, they are usually accompanied by specific anatomical changes like atrophy of the brain with reduced volume of the gray matter.
Now, moving on to clinical manifestations. Positive symptoms are those that occur “in addition” to normal experiences, therefore they are often referred to as “add-on” symptoms.
Clinical manifestations2:43–5:05
First, there are delusions, or strong false beliefs that the client might feel very strongly about even if there's strong evidence against it.
For example, clients with persecutory delusions believe that they are going to be harmed or harassed by other people; while in grandiose delusions clients believe that they are famous or have unnatural superpowers.
Next up are hallucinations, or perceptions of something in the real world that’s not really present. The most common type of hallucinations are auditory hallucinations, which involve hearing voices.
Less common are visual hallucinations, where clients see things that don’t exist; and tactile, olfactory, or gustatory hallucinations, when a person has a false perception of touch, smell, and taste.
Another important positive symptom is disorganized speech, which occurs because these individuals have difficulty controlling their flow of thoughts.
As a result, they switch from one conversation topic to another one with no connection or associations. Finally, there’s grossly disorganized or catatonic behavior, which can manifest as repetitive movements, unusual actions, bizarre posture, and not responding to other people's instructions.On the flip side, negative symptoms represent the absence of normal behavior and the most characteristic ones are called flat affect and anhedonia.
Flat affect manifests as decreased facial expressions, like frowning and smiling; reduced eye contact; and decreased speech intonation.
In addition, anhedonia is defined as the inability to enjoy pleasurable activities.Finally, these clients may present with cognitive problems, such as the inability to focus, impaired memory, and decreased ability to solve problems; or mood symptoms, such as depression, anxiety, and suicidal ideations.The diagnosis of schizophrenia is based on the client’s history and physical assessment.
Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a mental health condition.
Diagnosis5:05–6:14
Now, based on the DSM-5 criteria, schizophrenia is diagnosed in clients who present with at least two of the following symptoms over a one-month period: delusions, hallucinations, disorganized speech, disorganized or catatonic behavior, or negative symptoms.
But, it’s important to note that at least one of the symptoms has to be either delusions, hallucinations, or disorganized speech.Besides the one-month period which is required to meet the criteria, another criterion is that some symptoms should stick around for at least six months, either before, when they’re called prodromal symptoms, or after, when they’re called residual symptoms.
Additionally, lab testing can be used to assess if the client is intoxicated; while imaging methods can be used to exclude the presence of tumors in the central nervous system, which could potentially cause similar symptoms.Treatment of schizophrenia usually involves a combination of psychotherapy and pharmacotherapy.
Treatment6:14–7:08
Psychotherapy, including cognitive-behavioral therapy, focuses on teaching the client strategies to challenge negative thoughts, feelings, and behavior patterns.
In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Regarding pharmacotherapy, the first line medications are “atypical or second-generation” antipsychotics such as clozapine, risperidone, and olanzapine, which are better tolerated than the older “typical or first-generation” ones.
Finally, benzodiazepines might be administered to alleviate the anxiety some clients experience.Okay, let’s talk about the nursing care you would provide for a client with schizophrenia.
Management of care7:08–9:56
Your priority goals are to provide supportive care during symptom stabilization and maintain safety for the client and others.Starting with your assessment, evaluate your client’s mental status and level of anxiety.
If you notice that their eyes are darting around the room; if they seem preoccupied; if they are moving their lips silently; or if they are laughing at unusual times and appearing to have a one-sided conversation; they could be experiencing a hallucination.
Ask them if they are hearing voices or or seeing things. If they say they are, then ask them “What are the voices telling you?” or “What are you seeing?” to learn more about what they are experiencing.
Then, help your client by reassuring them that they are safe. Avoid overstimulating them, because this can make their anxiety worse and hallucinations more frightening and intimidating.
Instead, speak to them in a calm, reassuring voice using short and simple phrases, along with simple gestures. Keep in mind that your client is dealing with their own internal reality, so avoid interpreting their hallucination or discrediting their symptoms by using phrases such as “the voices aren’t real” or “they are all in your head.” Instead, help them focus on reality by saying something like “I know the voices you hear must be very upsetting for you, but I don’t hear the voices you’re talking about” or “I understand that must be frightening, but I don’t see any spiders on the wall.” Likewise, if your client is expressing a delusion, remember your client is unable to distinguish the difference between their delusion and reality.
Assist them by avoiding disagreeing or arguing with them about their delusion; and do not ask them to describe their delusion in more detail.
Instead, you could simply say, “I understand this is how you see things now,” and encourage them to talk about their anxiety or fears that are underlying the delusion.
Now, as your client’s symptoms begin to stabilize, continue to monitor them closely, administer the prescribed antipsychotic medications, and work with the psychiatric mental health team to maintain a safe, structured, therapeutic milieu.
If your client’s statements or behaviors indicate they are having suicidal or homicidal thoughts, immediately activate your facility’s safety protocol and report the client’s status to the healthcare provider.
Okay, moving on to client and family teaching. Begin by explaining that schizophrenia is a psychiatric condition that leads to problems with thinking and functioning in one or more areas of life.
General client & family teaching9:56–12:08
Then focus your teaching on symptom management and prevention of relapse. Stress the importance of adherence to their prescribed medications and participation in their ongoing cognitive behavioral therapy for rehabilitation.
Then review with them how to identify triggers that can increase anxiety, as well as strategies they can use for self-management of symptoms.
Encourage them to participate in activities that promote general well-being and reduce stress, such as meditation, mindfulness, and spending time on hobbies they enjoy.
Talk to them about lifestyle modifications such as getting adequate sleep, participating in physical activity, and eating a healthy, balanced diet.
Also review the benefits of making a daily schedule to manage their time, which will help prevent them feeling overwhelmed by tasks and deadlines.
Then, remind them to avoid the use of alcohol and recreational drugs and to talk to their healthcare provider before taking any over the counter medication or supplement, since these can change the way their medications work, and can make their symptoms worse.
Lastly, stress the importance of avoiding tobacco or other products that contain nicotine. Finally, teach the client and their family members to get help immediately if they are withdrawing from family or friends; if they have a significant change in mood and are feeling depressed, anxious, or agitated; if they talk about feeling hopeless or being a burden on others; if they talk about harming themselves or others; or if they are looking for a way to die by suicide, or talk about a specific suicide plan.All right, as a quick recap, Schizophrenia is a psychiatric condition caused by imbalanced dopamine levels in the brain.
Review12:08–13:32
Positive symptoms, also called “add-on” symptoms, include delusions, hallucinations, disorganized speech and grossly disorganized or catatonic behavior.
Negative symptoms include flat affect and anhedonia. Additionally, a client might experience cognitive and mood problems.Diagnosis is based on the DSM-5 criteria, and relies on having at least two of the following symptoms over a one-month period: delusions, hallucinations, disorganized speech, disorganized or catatonic behavior, or negative symptoms; with at least one of the symptoms being delusions, hallucinations or disorganized speech.
Besides the one-month period which is required to meet the criteria, another criterion is that some symptoms should stick around for at least six months.
Treatment relies on psychotherapy and medications like antipsychotics. Priority nursing goals are to provide supportive care during symptom stabilization and maintain safety for the client and others.
Client and family teaching focuses on learning about their disease, symptom management, prevention of relapse, and when to seek immediate medical attention.
| SCHIZOPHRENIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below