Shock - Obstructive: Nursing
Shock - Obstructive: Nursing
Watch later
Watch later
Notes
| SHOCK - OBSTRUCTIVE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Obstructive shock is a life-threatening condition that develops when a mechanical obstruction prevents the heart from filling properly or pumping enough blood through the cardiovascular system. This reduces the amount of oxygenated blood that reaches the tissues, causing acute hypoperfusion and tissue hypoxia.
Alright, let’s go over the physiology of the cardiovascular system, which consists of the heart and blood vessels. The heart pumps out blood to the body’s organs and tissues with each heartbeat, which consists of two phases: systole, which is when the heart contracts and pumps the blood out; and diastole, which is when the heart relaxes and fills with blood. The stroke volume, meaning the amount of blood pumped out by the heart in a single heartbeat, is influenced by the cardiac contractility, preload, and afterload. Contractility is how strongly the heart is contracting during systole. Preload is how much the heart’s smooth muscle is stretched at the end of diastole, and this is mainly dependent upon how much blood is filling the heart. The more they're stretched the more force they can generate during contraction, kind of like a rubber band. Afterload refers to the resistance that the heart must overcome to pump out blood during systole, and this is affected mainly by peripheral vascular resistance under non-pathological conditions. This is mainly determined by the vasodilation and vasoconstriction of blood vessels. If we multiply the stroke volume by the heart rate we’ll get the cardiac output, which is the amount of blood pumped out by the heart in one minute, and it’s the main measure of the heart’s function.
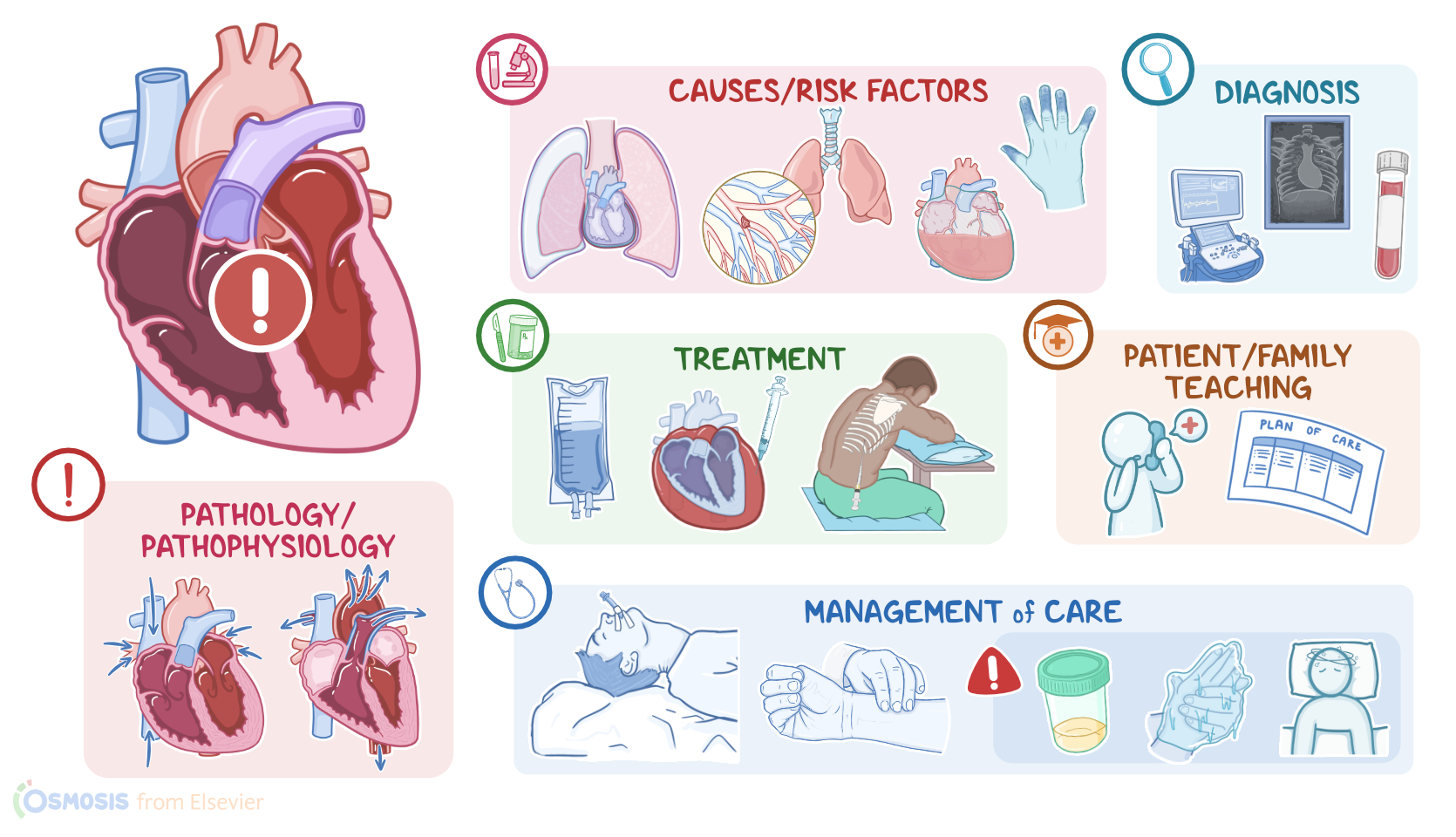
Okay, now obstructive shock is caused by an obstruction that prevents the heart from filling properly with blood during diastole, thus decreasing preload, or pumping blood out during systole, which increases afterload. One of the most common causes of obstructive shock is cardiac tamponade, where blood or fluid builds up in the pericardial sac, that surrounds the heart, preventing the heart from physically expanding during diastole. Another cause is constrictive pericarditis, where the pericardium becomes thickened and fibrotic, so it prevents the heart from expanding during diastole. Tension pneumothorax, where air builds up within the pleural space, increasing intrathoracic pressure which compresses the veins that return blood to the heart. Other causes that prevent the heart from pumping out blood effectively during systole include a massive pulmonary embolism, or blood clot, which blocks the flow of the blood that is pumped into the lungs, as well as conditions like aortic stenosis or coarctation of the aorta, which prevents blood from being pumped out during systole.
Now, the pathology of obstructive shock develops when a mechanical obstruction reduces blood flow into or out of the heart. As a result, there’s a decrease in stroke volume, which in turn decreases cardiac output, causing blood pressure to drop, and ultimately causing hypoperfusion of organs and tissues. So, in order to increase cardiac output, the body releases vasoconstrictor molecules into the bloodstream. These include catecholamines like epinephrine and norepinephrine which cause vasoconstriction, increase heart rate, and contractility to maintain blood pressure and blood flow; as well as ADH which acts on the kidneys to increase fluid retention, and angiotensin II, which also constricts blood vessels and causes sodium retention in the kidneys, in turn, raising blood pressure.
If the cause of shock is not managed in time, these compensatory mechanisms may begin to fail, leading to severe tissue hypoxia. Vital organs like the heart, brain, and kidneys may begin to shut down, leading to multiple organ failure. At the same time, since blood isn’t being pumped forward into the systemic circulation, it starts backing up into the pulmonary and systemic blood vessels. Eventually, fluid can be be pushed out of the circulation and into the lungs and tissues, leading to complications like pulmonary and peripheral edema.
Okay, during the initial stage, compensatory mechanisms such as increased heart rate and vascular constriction are sufficient to maintain cardiac output within the normal range. Cardiac output can best be seen by obtaining the mean arterial pressure, or the average pressure in one cardiac cycle, because it is a more accurate indicator of perfusion than a normal blood pressure. In this stage, the MAP is decreased by less than 10 mmHg from baseline. Clients may experience tachycardia, but compensatory mechanisms keep blood pressure at around the normal range, so it may be difficult to detect shock at this stage. During the compensation stage, the compensatory mechanisms are fully active but the MAP is decreased and is about 10-15 mmHg below baseline. The client’s skin can become cold and clammy, indicating that blood flow is being redirected to vital organs like the brain and heart. Other symptoms include pallor, severe hypotension and tachycardia, decreased peripheral pulses, and oliguria. Other important signs include pulsus paradoxus, where blood pressure during inspiration drops more than 10 mm Hg; as well as jugular venous distention, where the jugular vein in the neck becomes enlarged and distended. Lastly, some clients may develop pulmonary edema, which typically presents with dyspnea and crackles; as well as peripheral edema, causing the limbs to swell. In the progressive stage, clients can develop organ failure because the compensatory mechanisms can no longer guarantee adequate blood flow to vital organs. The MAP is sustained at more than 20 mmHg below baseline. The client may experience anxiety, altered level of consciousness from decreased perfusion to the brain, cyanosis, increased respirations, decreased oxygen saturation from lung failure, profound hypotension, bradycardia, and irregular heart rhythm from heart failure, as well as anuria, which occurs due to kidney failure. In the refractory stage, cell death occurs in the vital organs due to the lack of oxygen reaching the tissues. The MAP is still sustained at more than 20 mmHg from baseline. At this point, the damaged organs cannot respond to treatment, leading to multiple organ dysfunction. The client may experience a sudden loss of consciousness, shallow respirations, unmeasurable oxygen saturation, non-palpable pulses, or death.
The diagnosis of obstructive shock starts with the client’s history and physical assessment. The client should be monitored closely to detect signs of hypoperfusion, including a drop in oxygen saturation, low or declining blood pressure, sudden changes in the ECG, or decreased urinary output. This is usually followed by additional tests, including an echocardiogram, and a chest X-ray to identify the precipitating cause of obstructive shock. Routine diagnostic investigations also include laboratory tests that can reveal decreased oxygen levels, electrolyte abnormalities, and signs of end-organ damage like elevated lactate levels and metabolic acidosis.
Initial treatment of obstructive shock involves supportive measures, including supplemental oxygen, intravenous fluids, and medications like norepinephrine or dopamine to improve the cardiac output and blood pressure. However, definitive treatment is aimed at addressing the underlying cause of obstruction, when possible. This may include performing a pericardiocentesis to drain fluid from the pericardial space in cases of cardiac tamponade; draining excess air from the pleural space in tension pneumothorax; or treating a pulmonary embolism with anticoagulants and fibrinolytics, or removing a blood clot surgically via an embolectomy.