Venous thromboembolism (VTE): Nursing process (ADPIE)
Venous thromboembolism (VTE): Nursing process (ADPIE)
Respiratory System
Respiratory System
Notes
| VENOUS THROMBOEMBOLISM (VTE) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
Renata Gutierrez is a 34-year-old woman who came to the Emergency Department, or ED, with her partner, because of shortness of breath, chest pain, and coughing up blood-tinged sputum. The triage nurse informs you that Ms. Gutierrez delivered a healthy full-term baby by cesarean section one week ago. She has no other significant past medical history.
Venous thromboembolism, or VTE, refers to a clot that starts in a vein.
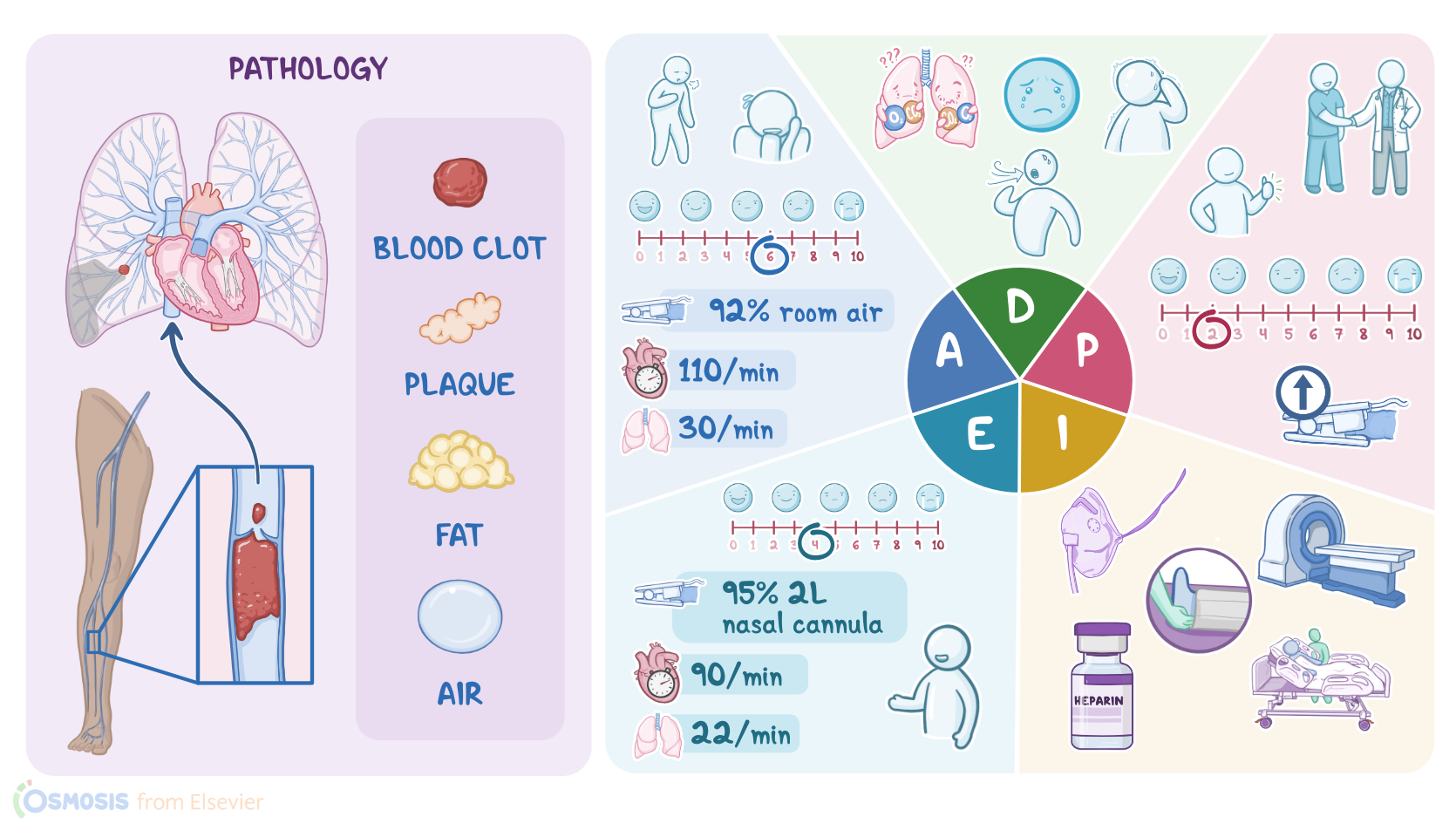
Specifically, a pulmonary embolism, or PE, occurs when an embolus, which is a small mass that could be a blood clot, fat, or even an air bubble, becomes lodged in the pulmonary artery and obstructs the pulmonary circulation. Most often the embolus is a blood clot associated with deep vein thrombosis, or DVT, which is when a clot forms in a large vein, usually in the leg or pelvis. The clot can break off and travel up the inferior vena cava to the right atrium, into the right ventricle, and finally into the pulmonary artery. This causes decreased blood flow to the lung tissue and impaired oxygenation.
Factors that increase the risk of a pulmonary embolism are summarized in Virchow triad, which include slowed blood flow, or venous stasis, hypercoagulation, meaning the blood is more likely to form clots, and damage to the endothelial lining of a blood vessel. Venous stasis can occur because of prolonged immobility like during a severe illness or after surgery, when an enlarged uterus compresses the nearby veins during pregnancy, or due to long-haul travel. Hypercoagulability can be caused by clotting disorders, use of oral contraceptives, smoking, and it occurs normally during pregnancy. And lastly, damage to the endothelial cell lining of a blood vessel can be the result of trauma or surgery.
Signs and symptoms of a pulmonary embolism depend on the size and location of pulmonary artery blockage. Even a small blockage impairs blood from getting into the lungs to pick up oxygen. Impaired oxygenation may cause a sudden onset of dyspnea, cough, tachypnea and chest pain that is described as pleuritic, meaning a sharp pain felt when inhaling and exhaling.
The patient may become disoriented and anxious from the hypoxemia, or they may report a feeling of apprehension and impending doom. As inflammation sets in, fluid buildup causes crackles which can be heard upon auscultation. Further deprivation of oxygen from the lung tissue leads to infarction of the lung tissue, which may result in hemoptysis. Complications from a PE can include pulmonary hypertension, right ventricular failure, shock and sudden death.
Diagnostics used to identify a PE include computed tomography pulmonary angiogram, or CTPA, where a dye is injected into the blood vessels to locate the blockage. A ventilation-perfusion scan, or V/Q scan, also called lung scintigraphy or ventilation-perfusion scintigraphy, can reveal areas of the lung that are ventilated, but not perfused, called a V/Q mismatch. Lab tests include a D-dimer test to detect fibrin breakdown products, which are usually present when there’s a blood clot.
Small clots may resolve on their own, however, large clots usually need treatment with fibrinolytic medications like tissue plasminogen activator, or tPA, to help break down the clot, and anticoagulants, like low molecular weight heparin to decrease blood coagulation. A
pulmonary embolectomy can also be done, either surgically or percutaneously, to remove the clot. For those at risk of developing further blood clots, anticoagulant medications may be given long term, or an inferior vena cava filter, or IVC filter, can be surgically placed into the inferior vena cava to prevent blood clots from entering the pulmonary artery and lungs. Keep in mind that the treatment course and medications may be influenced by factors such as whether the patient is pregnant or breastfeeding.
So, after you greet Ms. Gutierrez and introduce yourself as her nurse, you wash your hands, confirm her identity, and begin your assessment by asking how she’s doing. She replies she’s feeling short of breath, and it hurts every time she breathes. She goes on to tell you she has never experienced anything like this before and is very anxious. You notice that she has trouble getting the words out between breaths. After attaching a telemetry monitor, you observe sinus tachycardia with a heart rate of 110. Her respiratory rate is 30 per minute and shallow, she has a productive cough with blood-tinged sputum, and crackles are auscultated bilaterally. Her blood pressure is 95/72 mmHg, oral temperature 98.6° F, or 37°C, pain 6/10, and SpO2: 90% on room air.
Key Takeaways
Venous thromboembolism (VTE) is a condition where blood clots form in the veins, typically in the legs or pelvis, and can travel to the lungs, causing a pulmonary embolism (PE).
There are three main factors that lead to abnormal formation of clots, which are known as the Virchow's triad. They include venous stasis; a state of hypercoagulation; and damage to the endothelial cell lining. Venous stasis is said when blood doesn't flow appropriately in the veins due to prolonged periods of physical inactivity. Endothelial injury can occur when there is an injury or trauma to a blood vessel such as in trauma or surgery; and finally, hypercoagulable states can be seen in certain conditions like cancer and pregnancy.
Symptoms of VTE can include pain, swelling, warmth, and redness in the affected area, as well as shortness of breath, chest pain, and coughing up blood in the case of PE. The treatment involves thrombolytics to help break down the clot, or a thrombectomy, which is an intervention that aims to surgically remove the clot. Long-term treatment to prevent future thrombi from forming can include staying physically active, wearing compression stockings, and anticoagulant medications like warfarin or heparin.
Sources
- "Inflammation, Infection and Venous Thromboembolism. 128(12):2017-2036. " Circ Res. (2021)
- "Management of venous thromboembolism in pregnancy. 211:106-113. " Thromb Res (2022)
- "Long-term treatment of venous thromboembolism. 135(5):317-325. " Blood (2020)
- "Harrison’s Principles of Internal Medicine. 21st edition. ISBN: 978-1-264-26850-4 " McGraw Hill / Medical (2022)
- "Epidemiology and prevention of venous thromboembolism. 20(4):248-262. " Nat Rev Cardiol. (2023)
- "American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. 5(4):927-974. " Blood Advances. (2021)
- "Robbins & Kumar Basic Pathology. 11th edition. ISBN: 978-0-323-79018-5 " Elsevier (2022.)