Osteoporosis: Nursing
1,441visualizaciones
Notas
| OSTEOPOROSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcripción
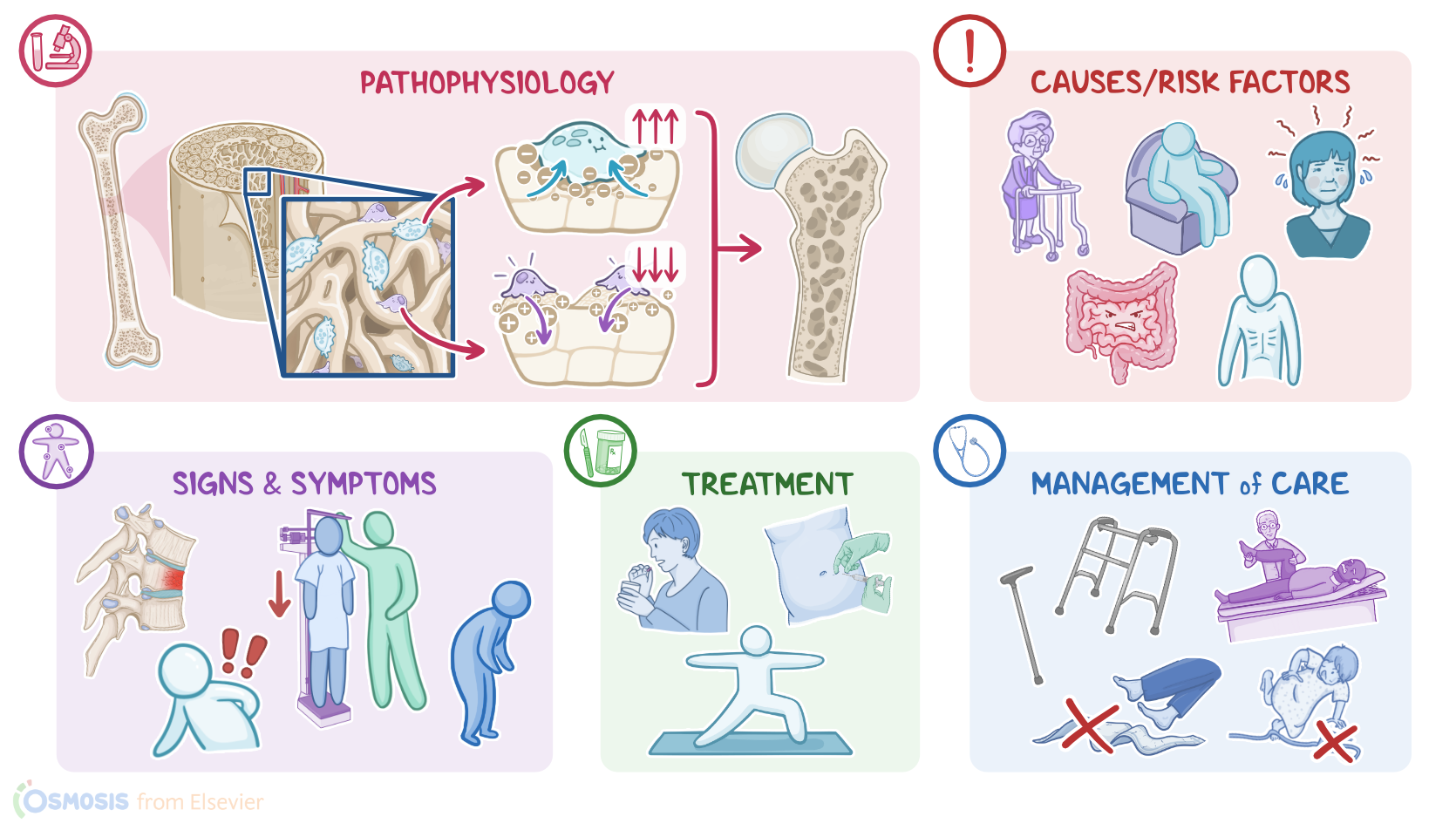
Osteoporosis is a chronic condition in which the bones gradually lose density or mass, becoming porous. This eventually leads to a decrease in bone strength, making the bones fragile and more prone to fracture with minimal trauma, or even spontaneously.
Now, most bones in the body have a dense external layer called compact bone; and a softer internal layer called spongy or trabecular bone, which normally consists of trabeculae and pores resembling a honeycomb. At first glance, a bone may appear inert and unchanging, but it’s actually a very dynamic tissue. In general, a bone is replaced with new cells every three to ten years in a process called bone remodeling, which has two steps: bone resorption, when specialized cells called osteoclasts break down bone, and bone formation, which is when another type of cells called osteoblasts form new bone.
Now, one of the main components of bones is calcium. For that reason, bone remodeling is highly dependent on blood calcium levels, which, in turn, are kept in the normal range by a balance between parathyroid hormone, or PTH, calcitonin, and vitamin D, as well as sex hormones. PTH is produced by the parathyroid glands in response to low blood calcium, and it increases bone resorption to release calcium from bones into the bloodstream. Vitamin D promotes calcium absorption in the gut, so it also increases blood calcium, promoting bone formation and decreasing bone resorption. On the other hand, calcitonin is produced by the thyroid gland in response to high blood calcium, so it opposes the action of PTH, therefore promoting bone formation and calcium deposition, while decreasing bone resorption. Finally, sex hormones like estrogen and androgens play a role by inhibiting bone resorption.
Now, there’s no specific cause of osteoporosis, but several risk factors that can accelerate bone mass loss. Modifiable risk factors include hormonal imbalances like hypogonadism or hyperthyroidism, malnutrition or dietary deficiencies including low calcium and vitamin D, excessive alcohol consumption, smoking, inadequate sun exposure, and sedentary lifestyle, as well as prolonged use of certain medications like glucocorticoids or antiepileptics like phenytoin. On the other hand, non-modifiable risk factors include family history of osteoporosis; ethnicity, especially Asian and Caucasian clients; aging, becoming particularly prevalent after 65 years of age; menopause; and certain conditions like hypogonadism, hyperprolactinemia, Turner syndrome, Klinefelter syndrome, Cushing syndrome, and diabetes mellitus. Additional non-modifiable risk factors include gastrointestinal conditions like inflammatory bowel disease, which can predispose clients to malnutrition.
So, the pathology of osteoporosis begins when the osteoclasts start breaking down the bones faster than the osteoblasts can rebuild. Over time, the bone density and mass gradually decrease, first leading to osteopenia, in which the decrease is still mild; at this point, bones become weaker than normal, but are still strong enough that they don’t break easily. Eventually though, if no preventive measures are taken, the compact bone thins out, while the spongy bone loses trabeculae and becomes more porous; at this point, osteopenia can progress to osteoporosis, where bones are so weak that they can break with minimal trauma or even spontaneously. These are called fragility fractures.
Now, clients with osteoporosis don’t usually have symptoms until a fragility fracture occurs. The most common type of fragility fractures are vertebral fractures, also known as compression fractures, which occur when one or more bones in the spine weaken and shatter. Vertebral fractures cause back pain, height loss, and a hunched posture. Other common fragility fractures that can occur include femoral neck or hip fractures and distal radius or wrist fractures.
The diagnosis of osteoporosis starts with history and physical assessment, followed by a dual-energy X-ray absorptiometry scan, or DEXA scan for short, to test for bone mineral density. The test compares an individual's bone density to that of a healthy adult, which yields the result as a T-score. A healthy client should have a T-score of -1 and above; while a T-score between -1 to -2.5 indicates that the client has osteopenia; and finally, a T-score of -2.5 or lower is diagnostic of osteoporosis.